After-hours clinical communication in a physician group practice depends on one accurate answer: which physician is on call right now? When a triage call arrives at the practice’s after-hours line at 11 p.m., the routing system must direct it to the nephrologist currently handling the call, not the physician who finished the call four hours ago. In a physician group rotating weekly coverage across multiple specialties, that resolution can fail more often than practice leadership realizes.
The consequences range from delayed responses to critical notifications reaching the wrong physician entirely. The Joint Commission identified communication failures as a leading cause of sentinel events in its 2024 Sentinel Event Data Annual Review, and the on-call handoff window is among the most vulnerable points in any clinical notification chain.
On-call schedule-aware routing eliminates this error class. By using the actual on-call schedule as a live data source for every routing decision, intelligent systems ensure that the right physician receives the right message at the right time. This article examines how the technology works, why independent physician groups with on-call obligations need it, and how ClinicianCore’s HCO Practice HQ delivers it.
Key Takeaways
- After-hours clinical notification errors in physician groups typically result from routing systems that do not update when on-call schedules change.
- When clinical support staff pages the on-call contact, the routing system must reflect who is actually carrying call at that moment, not who held it at the last manual update.
- The Joint Commission’s 2024 Sentinel Event Data Annual Review identified communication failures as a leading contributing cause of sentinel events, which increased 12% from 2023.
- HCO Practice HQ applies intelligent routing with role-based logic, real-time schedule awareness, and escalation rules that operate without manual intervention.
- Physician groups providing on-call coverage have the most to gain from automated routing, because the cost of a routing error in an acute clinical setting is immediate and patient-facing.
“The most dangerous assumption in a physician group practice is that the routing system knows who is on call right now. In most groups running static directories, it does not. On-call schedule-aware routing closes that gap before a misrouted page becomes a patient safety event.”

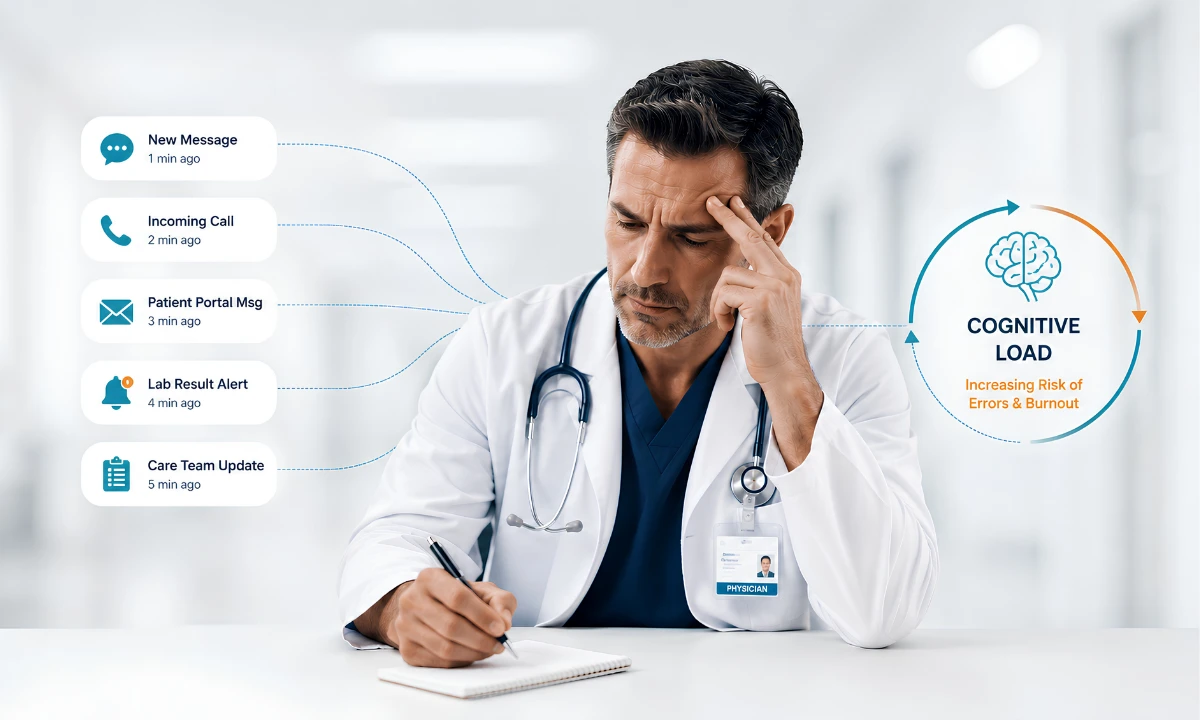
The Hidden Risk in After-Hours Clinical Notification
When a charge nurse in a clinical setting identifies a critical lab result at 11 p.m., a specific sequence must execute correctly: the notification enters the routing system, the system identifies the physician currently carrying a call for that patient population, and the page reaches the right contact. If step two fails, the clinical response is delayed before the on-call physician is even aware there is a situation requiring attention.
The failure most physician groups underestimate is in exactly that step. Physician groups rotating weekly call schedules across cardiology, nephrology, internal medicine, and surgical specialties generate frequent schedule changes. Coverage swaps happen when a physician has a conference commitment, a family obligation, or an unplanned illness. Each swap creates a window where the routing system reflects an outdated state.
The American Medical Association’s 2024 Physician Practice Benchmark Survey documents that 42.2% of physicians work in physician-owned independent practices, down from 60.1% in 2012. Many of these are specialty group practices that maintain on-call coverage as a core clinical obligation. These groups manage their own rotating call schedules, often with coverage changes communicated informally and rarely reflected in the routing system in real time.
AHRQ’s Patient Safety Network, updated in 2024, identifies communication failures during provider handoffs as among the most consistent causes of preventable medical errors. The on-call schedule transition is a handoff. When the outgoing physician’s contact remains in the routing system after their call window ends, every notification triggered during that period is a potential routing failure.
Why Static Routing Fails Physician Groups with On-Call Obligations
Static routing is any system where the on-call contact directory is updated manually. This includes clinical notification platforms where the on-call physician’s contact must be entered by a unit coordinator each shift, clinical communication systems with routing rules that require IT intervention to change, and scheduling overlays that are refreshed weekly rather than in real time.
All of these systems share the same structural vulnerability: they reflect the schedule as of the last manual update. A physician who swaps call with a colleague at 4 p.m. may not trigger a routing update until a coordinator processes the change the following morning. A locum tenens physician covering for a week may never be added to the notification directory. A physician who stepped off call due to illness may remain listed as the on-call contact for hours.
The notification chain that reaches on-call physicians runs through clinical support staff: the charge nurse who identifies the critical value, the unit coordinator who triggers the escalation, the clinical communication platform that routes the page. When the routing system carries the wrong contact, the error is invisible to the clinical staff initiating the notification. They send the page to the contact listed. The system is wrong. The page reaches a physician who is not carrying clinical responsibility at that moment.
The AMA reports that physicians logged an average 57.8-hour workweek in 2024, with 13 hours attributed to indirect patient care tasks, including documentation and test result interpretation, and 7.3 hours on administrative tasks. Receiving off-call pages because a routing system failed to update a schedule change adds unplanned interruptions to an already compressed schedule and compounds a burnout pattern the AMA has documented consistently across specialties.
What On-Call Schedule-Aware Routing Actually Does
On-call schedule-aware routing treats the on-call schedule as a live data object rather than a reference document. Instead of querying a static directory, the routing engine checks the schedule’s current state when a notification arrives, then identifies the physician or role currently assigned to receive that message type.
The operational difference is concrete. A static system asks: “Who is listed as the cardiology on-call contact?” A schedule-aware system asks: “Who is scheduled as the on-call cardiologist at this moment, for this coverage area?” The answer is drawn from a schedule that updates as coverage swaps are recorded, physicians rotate in and out of call duty, and on-call windows advance from one physician to the next.
This approach eliminates the most common routing failure patterns:
- Coverage-to-directory lag: the gap between when a schedule change is communicated and when the routing system reflects it.
- Role ambiguity: when multiple physicians share an on-call designation and the system cannot determine which is currently active.
- Escalation gaps: when the primary on-call physician is unreachable and there is no automated pathway to the backup.
For physician groups, schedule-aware routing also resolves a documentation gap. Every notification delivered through a schedule-aware system is tied to a specific on-call assignment at a specific time. This creates an auditable record of who received what message, when, and under what routing rule.
How Intelligent Routing Goes Beyond Schedule Lookup
Schedule awareness alone, implemented as a lookup of the current on-call schedule, is a meaningful improvement over static directories. Intelligent automation extends this capability across three additional dimensions: urgency scoring, pattern recognition, and adaptive escalation.
Urgency scoring applies a classification model to each incoming notification to determine its time sensitivity. A critical lab value for a patient with a history of renal failure is not the same urgency class as a non-urgent clinical documentation task. intelligent routing systems classify the incoming notification against its content, the clinical parameters of the patient, and the context of the sending provider, then route accordingly. High-urgency classifications trigger immediate delivery to the on-call physician. Lower-urgency classifications are queued for next-available response, reducing unnecessary interruption while ensuring nothing critical is deferred.
Pattern recognition allows the routing system to learn from its own history. Which notification types from which clinical units consistently require on-call physician engagement? Which are consistently resolved by nursing without escalation? Over time, the routing model improves its accuracy for a specific group’s workflow patterns, reducing both over-alerting and under-alerting.
Adaptive escalation handles the scenario that static routing cannot address: the non-response. When the on-call physician does not acknowledge an urgent notification within a defined window, the system escalates automatically to the backup on-call contact, then to the senior attending if needed. This escalation chain operates without manual intervention, removing the burden from clinical support staff who would otherwise need to make multiple calls to locate a responding physician.
Intelligent routing is not about replacing physician judgment. It is about ensuring that physician judgment is applied to the right messages, at the right time, by the right physician. ClinicianCore’s healthcare AI and innovation platform is built on this principle.
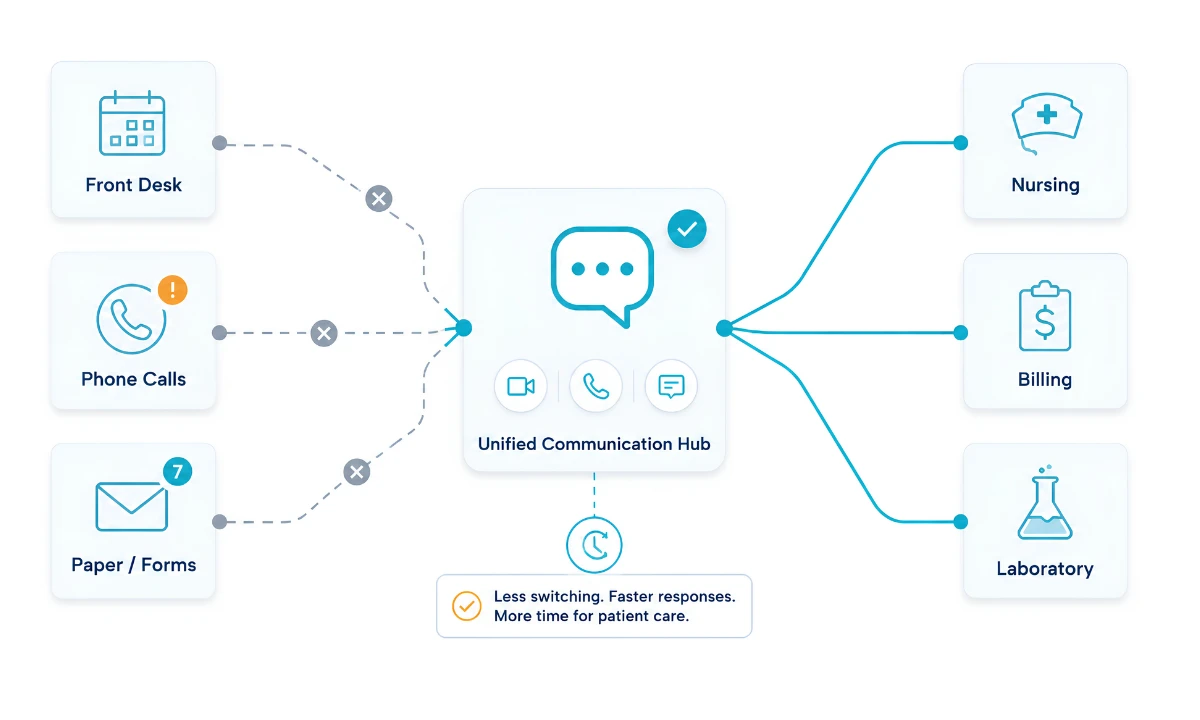
ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, applies these capabilities specifically to the routing challenges faced by independent physician groups with after-hours call obligations.
HCO Practice HQ: Schedule-Aware Routing for Physician Groups
HCO Practice HQ is the organizational communication layer within ClinicianCore. Its Intelligent Routing feature is purpose-built for the schedule-aware routing problem that physician groups with on-call obligations face.
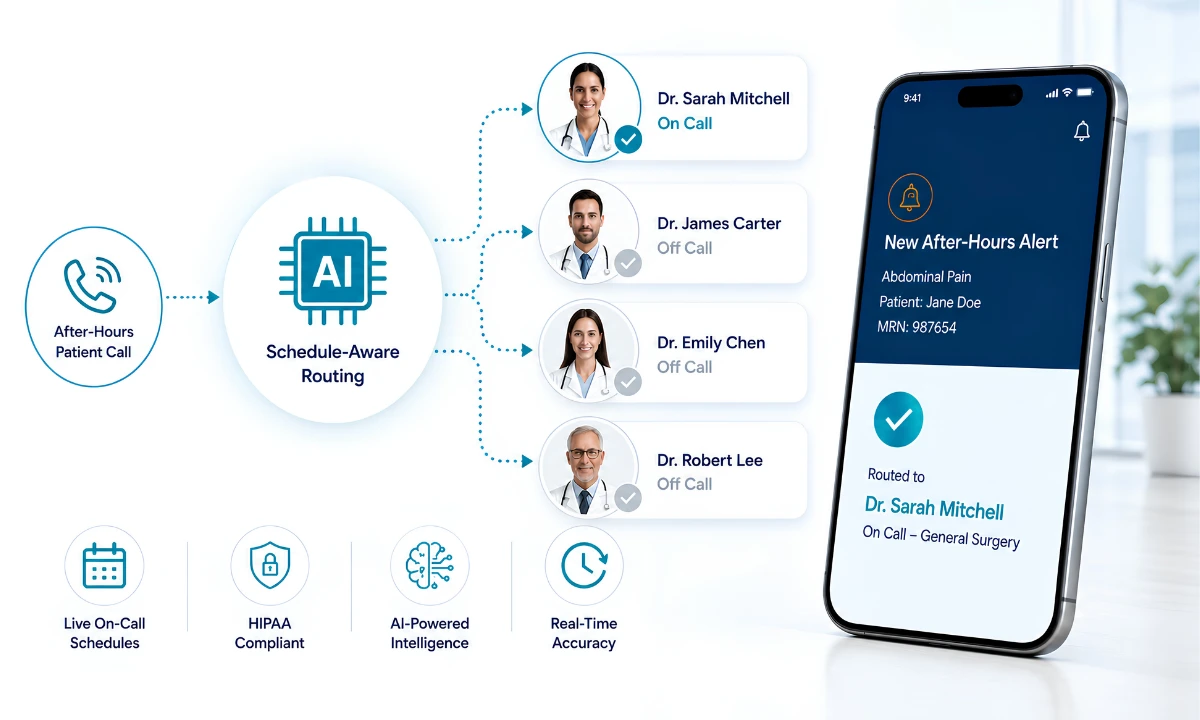
The feature operates on a role-based routing architecture. Each notification enters the system with a destination role rather than a destination contact name. The system resolves that role to the specific physician who holds it on the current schedule. A notification designated for the nephrology on-call role reaches whoever is currently assigned to that role, not whoever was last manually entered in a directory.
As a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, HCO Practice HQ encrypts every message in transit and at rest, maintains a complete audit trail by physician and by routing rule, and ensures that no notification is delivered through an unencrypted channel regardless of the hour or urgency. This is particularly relevant where clinical support staff may default to consumer messaging applications when standard channels appear to fail, creating HIPAA exposure that a properly routed system eliminates. The broader notification overload problem that intelligent routing addresses at the organizational level is covered in detail in the alert fatigue in healthcare article.
On-call schedule integration works through a direct sync with the group’s scheduling system. When a physician is added to or removed from call duty, routing rules update within seconds. Coverage swaps processed by a scheduling coordinator reflect immediately in routing behavior, eliminating the lag that creates the static routing failure window.
Escalation rules are configured at the group level. The group defines which urgency classes trigger immediate delivery, what the response window is before escalation begins, and who holds the backup position for each on-call role. These configurations persist across schedule rotations, so each new on-call physician inherits the correct escalation structure without any manual setup.
Physician groups planning their routing implementation can review the module’s full capability on the HCO Practice HQ platform page and join the waitlist for the September 2026 launch.
The Patient Safety Case for Getting Routing Right
The clinical stakes of after-hours routing failures are documented in patient safety data. The Joint Commission’s Sentinel Event Data 2024 Annual Review reported 1,575 sentinel events, a 12% increase over 2023, with failures in communication and consistently following policies identified as leading contributing causes.
AHRQ’s Patient Safety Network, in a primer reviewed and updated in 2024, documents that ineffective communication during provider handoffs is consistently associated with increased medical error rates across settings from emergency departments to intensive care units. The on-call schedule transition is a handoff. When one physician’s call window ends and another begins, there is a communication transition with all the risk that patient safety research has documented for decades.
Independent physician groups carry this risk without the redundant notification systems that large health institutions maintain. A major health system may have clinical pharmacists, charge nurses, and attending physicians all available after hours to catch a misrouted critical notification. A six-physician specialty group covering after-hours call has the on-call physician and whoever clinical staff can reach if the first contact fails.
The Physicians Foundation’s 2024 Survey of America’s Current and Future Physicians found that six in ten physicians reported often experiencing burnout. After-hours communication burden, including receiving off-call pages because the routing system was not updated, is a documented contributor to that burden. Physician burnout reduction and communication system accuracy are not separate problems. A routing failure that delivers an off-hours page to the wrong physician is simultaneously a patient safety event and a practice retention risk.
Building a Routing Strategy for Your Physician Group
Implementing schedule-aware intelligent routing begins with an audit of how after-hours clinical notification currently flows. Before adopting any new system, the group should map who is responsible for updating on-call contact information in the routing system, what the process is for recording a coverage swap, how quickly schedule changes propagate to the notification platform, and how escalation currently works when the on-call physician does not respond.
This audit typically reveals two findings. First, the gap between the schedule as recorded and the schedule as it actually stands is larger than group leadership expects, because informal swaps and last-minute coverage changes are rarely captured in routing systems in real time. Second, the escalation process is usually manual, meaning that when a critical page goes unanswered, clinical staff must work through a backup contact list by phone.
With that baseline documented, the group can define its routing requirements: how many distinct on-call roles exist by specialty and urgency tier, what the response window is before escalation, who holds the backup position for each role, and how the system should handle the transition window when one on-call physician hands off to the next. In HCO Practice HQ, these specifications are configured once and persist across all future schedule rotations.
The HIPAA compliance layer is non-negotiable. Every notification that contains or references protected health information must travel through a HIPAA-compliant channel, regardless of urgency or time of day. ClinicianCore’s platform, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, provides end-to-end encryption and role-based access controls across every device and every shift. Physician groups that currently allow clinical staff to send on-call notifications through consumer applications are operating with open HIPAA exposure that a structured routing platform closes. For a detailed view of the compliance requirements, see ClinicianCore’s HIPAA-compliant collaboration platform and medical practice efficiency resources.
Three Steps to Start This Week
- Document your current routing accuracy. Ask the on-call physician to log every page they receive over two weeks that should have gone to a colleague. The number will be higher than practice leadership expects.
- Map your escalation chain. Write down the exact process that triggers when the on-call physician does not respond within fifteen minutes. If that process exists only in a coordinator’s memory, it is not a reliable process.
- Evaluate your routing platform. Is the current notification system schedule-aware, or is it operating from a static directory? Does it update in real time when coverage changes, or does it require a manual entry? The answer determines whether your group has a routing system or a routing problem.
Frequently Asked Questions
What Is Schedule-Aware Routing in Clinical Communication?
On-call schedule-aware routing uses the current on-call schedule as a live routing source, not a static directory. The system identifies which physician holds the relevant on-call role at a given moment and routes accordingly. AHRQ (2024) identifies handoff communication failures as a consistent driver of preventable medical errors. ClinicianCore’s HCO Practice HQ delivers this capability to independent practices.
How Does On-Call Routing Failure Contribute to Medical Errors in Physician Practices?
On-call routing failures direct urgent clinical notifications to physicians not currently carrying call, creating response delays in time-sensitive situations. The Joint Commission’s 2024 Sentinel Event Data Annual Review identified communication failures as a leading contributing cause of sentinel events, which rose 12% from 2023. Correctly routing after-hours notifications prevents a preventable subset of these events.
What Features Should Physicians Look for in an Intelligent Clinical Routing System?
Physicians evaluating intelligent clinical routing systems should look for real-time on-call schedule integration, role-based routing that resolves automatically to the current on-call physician, configurable escalation rules with defined response windows, and end-to-end HIPAA compliance. The AMA (2024) reports a 57.8-hour physician workweek; eliminating misrouted alerts is a direct efficiency gain that protects clinical capacity.
How Does On-Call Schedule-Aware Routing Differ from Traditional Paging Systems?
Traditional paging routes to a static contact requiring manual updates when coverage changes. On-call schedule-aware routing resolves the destination from the live on-call schedule, without manual intervention. The Physicians Foundation’s 2024 Survey found six in 10 physicians report burnout. Eliminating misrouted after-hours notifications reduces a documented contributor to that clinical burden.
Is HIPAA-Compliant Routing Possible for After-Hours Physician Communication?
HIPAA-compliant after-hours routing requires all notifications with protected health information to travel through encrypted channels with access controls restricting visibility to authorized providers. ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, providing end-to-end encryption and audit logging as standard features. Consumer messaging apps used for on-call communication create reportable HIPAA exposure.
References
[1] American Medical Association. Physician burnout rate continues to decline, falling to nearly 42%. American Medical Association; 2026. https://www.ama-assn.org/practice-management/physician-health/physician-burnout-rate-continues-decline-falling-nearly-42
[2] American Medical Association. Doctors work fewer hours, but the EHR still follows them home. American Medical Association; 2025. https://www.ama-assn.org/practice-management/physician-health/doctors-work-fewer-hours-ehr-still-follows-them-home
[3] American Medical Association. Digging into the data to cut EHR burdens that drive burnout. American Medical Association; 2024. https://www.ama-assn.org/practice-management/digital-health/digging-data-cut-ehr-burdens-drive-burnout
[4] The Joint Commission. Sentinel Event Data 2024 Annual Review. The Joint Commission; 2025. https://www.jointcommission.org/resources/patient-safety-topics/sentinel-event/
[5] The Joint Commission. Sentinel Event Data 2023 Annual Review. The Joint Commission; 2024. https://www.jointcommission.org/resources/patient-safety-topics/sentinel-event/
[6] AHRQ Patient Safety Network. Handoffs. Agency for Healthcare Research and Quality; 2024. https://psnet.ahrq.gov/primer/handoffs
[7] American Medical Association. Physician Practice Benchmark Survey. American Medical Association; 2024. https://www.ama-assn.org/about/ama-research/physician-practice-benchmark-survey
[8] The Physicians Foundation. 2024 Survey of America’s Current and Future Physicians. The Physicians Foundation; 2024. https://physiciansfoundation.org
[9] Choudhary A, Adhikari S, White PC. Implementation of After-Hours Nurse Line in an Academic Pediatric Endocrinology Practice. Published September 11, 2023. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12017214/
[10] Murad DA, Tsugawa Y, Elashoff DA, Baldwin KM, Bell DS. Distinct components of alert fatigue in physicians’ responses to a noninterruptive clinical decision support alert. J Am Med Inform Assoc. 2023;30(1):64-72. https://academic.oup.com/jamia/article-abstract/30/1/64/6764683