During my years as a surgeon in the Air Force, I learned something that applies to every clinical environment I have worked in since: you cannot make precise decisions under constant noise. In the operating room, we protect against interruptions deliberately. The room quiets. Tasks are sequenced. The cognitive environment is guarded because the consequences of distraction are immediately visible.
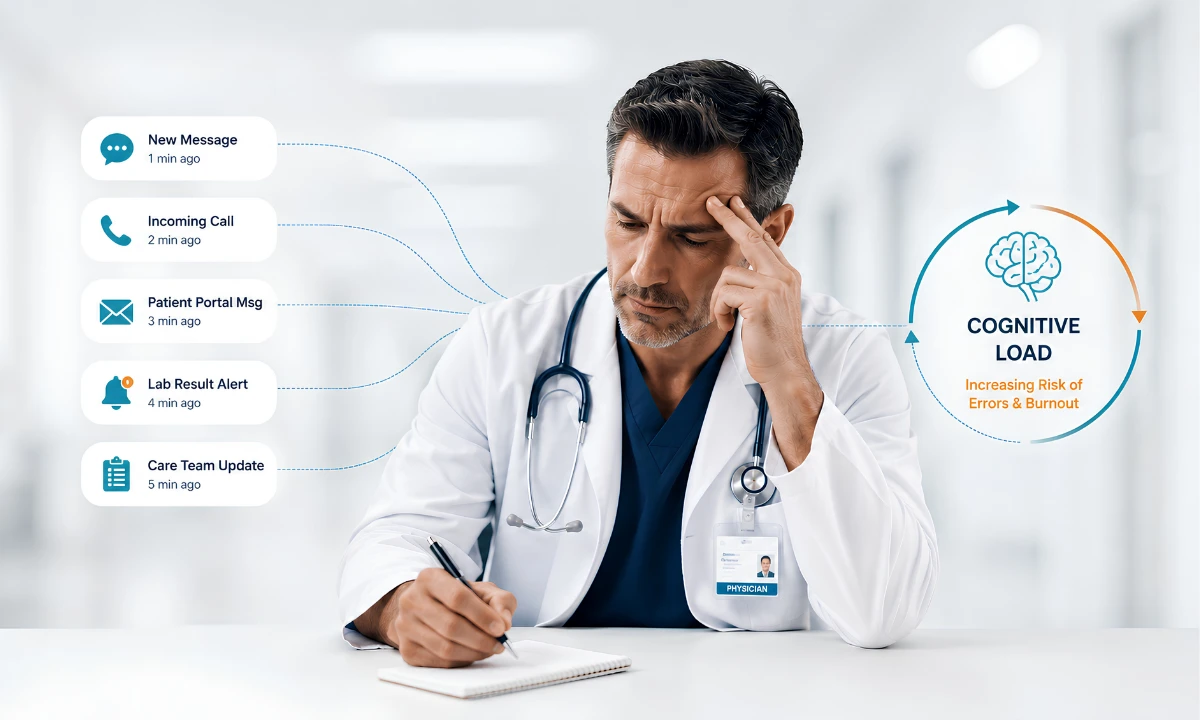
The cognitive cost of clinical interruptions extends far beyond a momentary distraction. Every unnecessary page, alert, or message forces physicians to suspend clinical reasoning, rebuild working memory, and recover cognitive focus before safe decision-making can resume.
In the exam room, the call room, and the hallway between patients, the interruptions are just as frequent, and the consequences just as real. What differs is that we rarely protect against them with the same deliberateness.
Research has given us the cognitive science to explain what physicians have always felt: every interruption costs more than the seconds it takes to field it. It disrupts working memory, forces task-switching, and requires meaningful mental effort to re-establish the reasoning state that existed before the intrusion arrived.
Communication overload is not an inconvenience. It is a patient safety issue and a primary contributor to the physician burnout crisis persisting across American medicine. This post examines what the evidence shows and what a structural response looks like for independent physician group practices.
Key Takeaways
- Emergency physicians face an average of 10 interruptions per hour; research shows 57% of clinical interruptions are avoidable. (Teigné et al., Int J Qual Health Care, 2023)
- Interruptions are significantly associated with increased medication error rates, documented in both JAMA Pediatrics (2020) and Archives of Internal Medicine (2010).
- Every interruption creates a “resumption lag” — the cognitive work required to re-establish clinical reasoning — directly elevating error risk during high-stakes tasks.
- The American Medical Association found 43.2% of physicians reported at least one burnout symptom in 2024, with communication overload cited among top stressors. (AMA, 2024)
- Intelligent routing reduces the 57% of avoidable interruptions that drive preventable cognitive burden without compromising urgent clinical communication.
“Communication overload is not an inconvenience. It is a patient safety issue and a structural contributor to physician burnout.”

The Cognitive Science Behind Clinical Interruptions
Cognitive load theory provides the framework for understanding why interruptions are so reliably harmful.
Understanding the cognitive cost of clinical interruptions begins with recognizing that every disruption consumes limited mental resources that physicians rely on for diagnosis, prioritization, and clinical judgment.
The human working memory has limited capacity. When that capacity is overwhelmed by competing demands, performance does not degrade gradually. It drops.
In clinical settings, physicians operate under high intrinsic cognitive load: the mental work of diagnosis, differential reasoning, and real-time decision-making. Every incoming alert, page, or unscheduled message adds what cognitive scientists call “extraneous load” — demand that contributes nothing to the clinical task but consumes the same limited cognitive resources. A 2024 narrative review published in JMIR Medical Informatics confirmed that cognitive overload occurs when working memory’s capacity is exceeded through excessive information processing, and that this overload has measurable effects on clinical performance and physician well-being. [1]
What matters here is the specific mechanism. When a physician is interrupted during clinical reasoning, they do not simply pause. They must suspend the active goals of the primary task, encode and process the interrupting task, and then reconstruct where they were before the interruption arrived. Cognitive researchers call the time required for this reconstruction the “resumption lag.” In complex clinical reasoning, that lag is the window in which errors are most likely to occur.
The structural problem is that most communication environments in physician group practices do not account for this cognitive reality. Every alert arrives with the same urgency weighting, placing the entire burden of triage on a physician whose working memory is already engaged with active clinical demands.
How Often Are Physicians Actually Interrupted During a Clinical Shift?
The frequency data is difficult to absorb without a clinical frame.
Emergency physicians face an average of 10 interruptions per hour, or once every six minutes, according to a perspective on interruptions and patient safety published on AHRQ’s Patient Safety Network. [2] A 2023 observational study in the International Journal of Quality in Health Care examined 23 care teams across 17 clinical sites and found that professionals were interrupted an average of 10.5 times per hour. Critically, the same study found that 57 percent of those interruptions were classified as avoidable. [3]
That 57-percent figure matters more than the raw frequency count. It means that more than half of the cognitive disruption physicians absorb each shift is not clinically necessary. It arrives because the communication infrastructure treats every message with equal urgency. The routing logic to distinguish a time-sensitive alert from a routine administrative notification either does not exist or is not enforced.
For independent physician group practices, this dynamic is compounded by staffing structure. There is no administrative buffer absorbing non-urgent communication before it reaches the physician. Notifications land directly, and the cognitive cost accumulates across every patient encounter in a shift.
A secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians addresses this gap not by blocking communication but by routing it intelligently, so that only what is clinically urgent reaches the attending physician in real time. Join the ClinicianCore waitlist to see how intelligent routing works in practice.
When Do Clinical Interruptions Become Medical Errors?
The cognitive cost of clinical interruptions becomes most apparent when repeated disruptions interfere with medication administration, diagnostic reasoning, or other high-consequence clinical tasks where sustained attention is essential. The research connecting interruptions to clinical harm has moved well beyond correlation.
A 2010 study published in the Archives of Internal Medicine directly observed nurses at two major teaching hospitals preparing and administering medications. The study found that interruptions were significantly associated with both the frequency and severity of medication administration errors. The more frequently a nurse was interrupted, the higher the rate of procedural failures, and the greater the clinical severity of those failures. [4]
A decade later, a prospective cohort study published in JAMA Pediatrics examined 257 nurses administering more than 238,000 medication doses in a pediatric intensive care unit over 12 months. Incoming mobile telephone calls within 10 minutes of medication administration were associated with a statistically significant increase in error rates. When nurses were not interrupted, the error rate was 3.1 percent. With mobile phone interruptions, that rate rose to 3.7 percent. [5]
AHRQ’s Patient Safety Network cites observational research showing that two-thirds of clinical interruptions delay the original task, and one-fourth result in a loss of concentration or focus. [2] What the data cumulatively describe is a system-level failure: communication channels that deliver every notification to the clinician without distinguishing between what is urgent and what is not. The physician bears the cognitive cost of every message, regardless of its clinical priority.
alert fatigue in independent physician practices
The Burnout Connection
The cognitive drain from interruptions accumulates across shifts, months, and years. At some point, it stops being a daily inconvenience and becomes the kind of sustained depletion that drives physicians toward career exit.
The cumulative cognitive cost of clinical interruptions is one of the structural drivers of physician burnout because clinicians repeatedly expend mental energy recovering from unnecessary task switching throughout the workday.
The American Medical Association’s 2024 national physician comparison report found that 43.2 percent of physicians reported at least one symptom of burnout, with ineffective EHR systems, excessive in-basket volume, and administrative tasks cited among the top sources of professional stress. [6] The Physicians Foundation’s 2024 Survey of America’s Current and Future Physicians found that six in ten physicians often have feelings of burnout — a rate that has remained consistently elevated since 2020. [7]
A BMJ Quality and Safety study confirmed the mechanistic link: task errors by emergency physicians were directly associated with interruptions, multitasking, and cognitive fatigue. The study found that working memory capacity moderated the relationship between interruption frequency and error rates — physicians with lower available cognitive reserve made more errors when interrupted. [8] The cognitive resource that protects against burnout and against clinical errors is the same resource.
What this means for practice is that the interruption problem is not separable from the burnout problem. Addressing one requires addressing the other.
For physicians committed to sustainable practice, the structural pathway begins with reducing the volume of avoidable interruptions that consume cognitive reserves before a single clinical decision is made. Our physician burnout reduction platform is built on exactly this framework: protecting physician cognitive resources through structured, intelligent communication.
Not All Interruptions Are Equal
The solution to the interruption problem is not silence. Critical alerts must reach the attending physician without delay. The clinical stakes of a missed urgent notification are just as real as the cognitive costs of unnecessary ones.
What the research supports, and what the 57-percent avoidable rate underscores, is that the problem is not the volume of communication. It is the absence of clinical context in how that communication is routed.
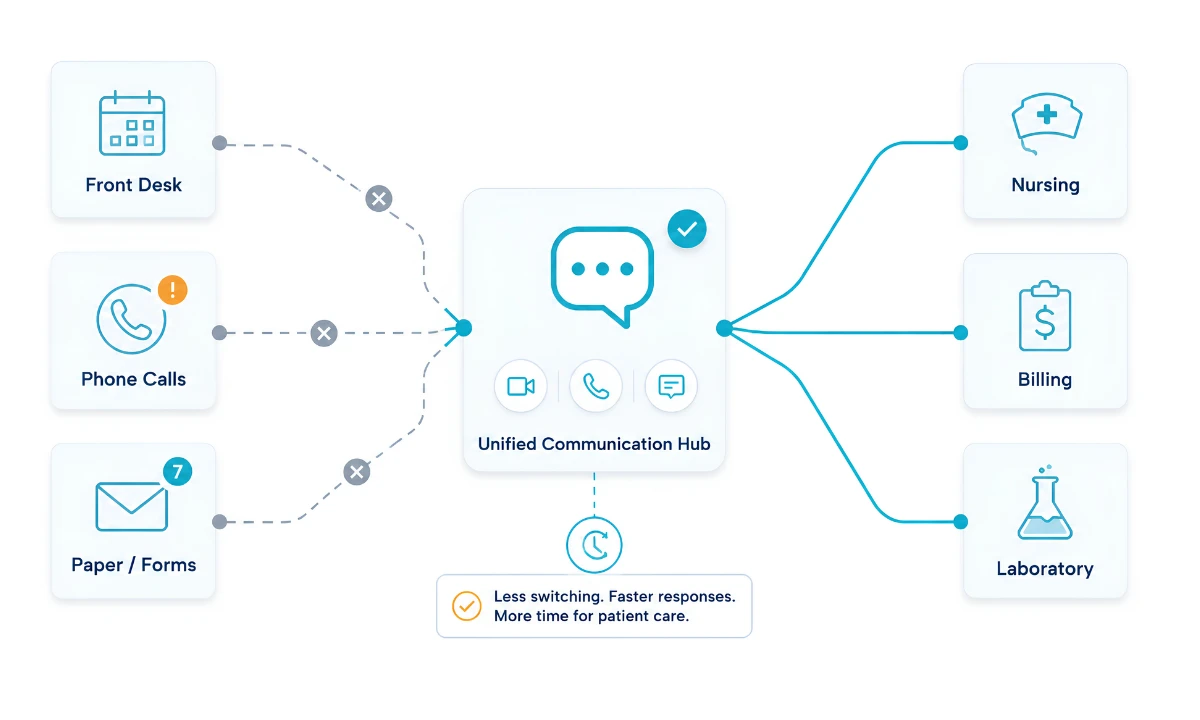
Unified Clinical Communication provides the structural foundation for reducing unnecessary clinical interruptions by bringing secure messaging, voice, video, alerts, and clinical collaboration into a single coordinated communication environment. Instead of forcing physicians to monitor multiple disconnected applications, a unified platform establishes shared clinical context, prioritizes communication based on urgency, and ensures that the right information reaches the right clinician at the right time. This systems-based approach reduces cognitive burden while improving physician efficiency, patient safety, and care team collaboration.
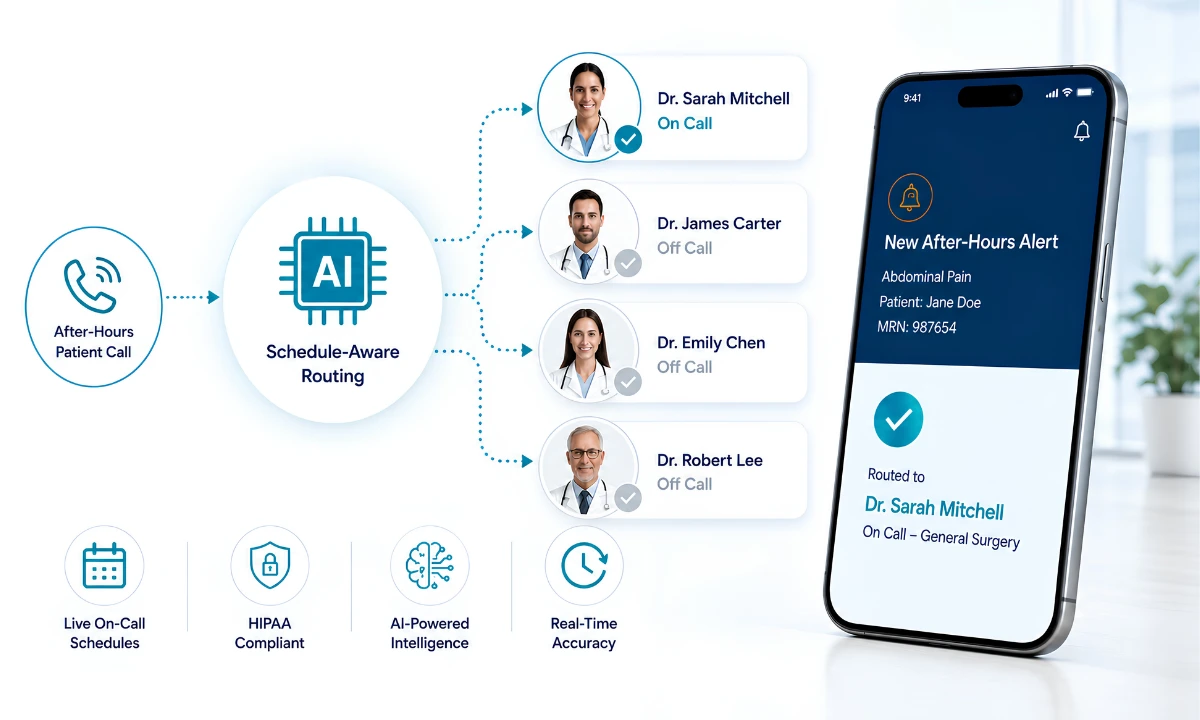
Intelligent routing is the technology-driven process of filtering, prioritizing, and escalating messages based on urgency classification, on-call status, and clinical role. Rather than delivering every notification to the attending physician in parallel, a well-configured routing system directs routine updates to the appropriate staff member, escalates based on predefined urgency thresholds, and ensures that the physician’s real-time queue contains only what requires immediate clinical judgment.
A platform built and operated as a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians can maintain this routing context across a full clinical shift, adapting to on-call rotations, specialty role assignments, and urgency parameters, without placing the triage burden back on the physician.
HIPAA-compliant messaging for independent physician groups
From Research to Practice: What Independent Physician Groups Can Do
For independent physician group practices, the path from awareness to structural change is more direct than it may appear.
Reducing the cognitive cost of clinical interruptions requires more than asking physicians to ignore distractions. It requires communication systems that prioritize, route, and escalate information according to genuine clinical urgency.
The diagnostic step is straightforward: audit one week of incoming notifications across the practice. Classify each by urgency and intended recipient. In nearly every practice that has completed this exercise, the distribution is consistent with what the research shows: more than half of physician-directed notifications should have routed elsewhere.
The structural response to that audit is where communication infrastructure becomes determinative. HCO Practice HQ, part of a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, applies role-based routing logic and urgency classification across the practice’s communication environment. Alerts are classified before they reach the physician. Routine administrative messages route to clinical staff. Urgent notifications escalate through predefined protocols. The physician’s notification queue narrows to what is clinically necessary.
Practices that implement structured routing report benefits beyond cognitive relief. When physicians receive fewer but higher-quality interruptions, their confidence in the notification system increases. Non-urgent messages stop being ignored because they are no longer competing with urgent alerts for attention in a shared queue. The communication environment becomes functional rather than noisy.
This is the medical practice efficiency dimension of the interruption problem: the cognitive cost of unmanaged communication does not stay contained to the physician’s experience. It affects throughput, documentation quality, and the completeness of clinical decision-making across the practice. Addressing it produces operational returns alongside the patient safety and physician well-being outcomes that the research documents.
Reducing the cognitive cost of clinical interruptions is ultimately a systems challenge rather than an individual physician challenge. Practices that redesign communication around clinical priority create safer workflows, lower cognitive burden, and stronger foundations for physician well-being.
Physicians ready to move from awareness to action can join the ClinicianCore waitlist and see intelligent routing in an independent physician group practice context.
Frequently Asked Questions
What is cognitive overload in physicians and how does it affect patient care?
Cognitive overload in physicians occurs when working memory’s limited capacity is exceeded by competing information demands, impairing clinical reasoning and decision-making. A 2024 narrative review in JMIR Medical Informatics confirmed that cognitive overload has measurable effects on clinical performance. Communication interruptions are a primary driver, directly increasing the risk of medical error.
How many times per hour are physicians interrupted in a clinical setting?
Emergency department physicians face an average of 10 interruptions per hour, or once every six minutes, according to AHRQ’s Patient Safety Network. A 2023 observational study found that clinical teams were interrupted 10.5 times per hour on average, with 57 percent of those interruptions classified as avoidable.
Can clinical communication technology reduce interruption-related medical errors?
Research supports that reducing interruption frequency during high-stakes clinical tasks reduces error rates. A study in JAMA Pediatrics found that mobile phone interruptions during medication administration raised error rates from 3.1 to 3.7 percent. Intelligent routing that prevents non-urgent notifications during active tasks is the targeted intervention the evidence supports.
What is the connection between clinical interruptions and physician burnout?
Clinical interruptions drain the working memory physicians need for complex reasoning. The AMA’s 2024 national physician comparison report found 43.2 percent of physicians reported at least one burnout symptom, with EHR inefficiency and administrative overload as top stressors. Reducing avoidable interruptions is among the strongest evidence-supported interventions available to independent physician practices.
What should independent physician group practices do to reduce interruption-related cognitive overload?
Independent physician group practices should first audit their interruption volume, categorizing each notification as urgent, non-urgent, or misrouted. Research shows that 57 percent of clinical interruptions are avoidable. The structural intervention is routing logic that prevents non-urgent alerts from reaching the attending physician during active tasks.
References
[1] Asgari E, Kaur J, Nuredini G, et al. Impact of Electronic Health Record Use on Cognitive Load and Burnout Among Clinicians: Narrative Review. JMIR Med Inform. 2024;12:e55499. doi:10.2196/55499. https://medinform.jmir.org/2024/1/e55499
[2] Agency for Healthcare Research and Quality. Interruptions and Distractions in Health Care: Improved Safety With Mindfulness. AHRQ Patient Safety Network Perspectives. https://psnet.ahrq.gov/perspective/interruptions-and-distractions-health-care-improved-safety-mindfulness
[3] Teigné D, Cazet L, Birgand G, et al. Improving care safety by characterizing task interruptions during interactions between healthcare professionals: an observational study. Int J Qual Health Care. 2023;35(3):mzad069. doi:10.1093/intqhc/mzad069. Cited in AHRQ PSNet: https://psnet.ahrq.gov/issue/improving-care-safety-characterizing-task-interruptions-during-interactions-between
[4] Westbrook JI, Woods A, Rob MI, Dunsmuir WTM, Day RO. Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med. 2010;170(8):683-690. doi:10.1001/archinternmed.2010.65
[5] Bonafide CP, Miller JM, Localio AR, et al. Association Between Mobile Telephone Interruptions and Medication Administration Errors in a Pediatric Intensive Care Unit. JAMA Pediatr. 2020;174(2):162-169. doi:10.1001/jamapediatrics.2019.5001. https://pmc.ncbi.nlm.nih.gov/articles/PMC6990809/
[6] American Medical Association. U.S. physician burnout hits lowest rate since COVID-19. AMA National Physician Association Between Mobile Telephone Interruptions and Medication Administration Errors in a Pediatric Intensive Care Unit – PMC Comparison Report, 2024. https://www.ama-assn.org/practice-management/physician-health/us-physician-burnout-hits-lowest-rate-covid-19
[7] The Physicians Foundation. Examining Physician, Resident and Student Wellbeing and Impact of the Current Healthcare Landscape. 2024 Survey of America’s Current and Future Physicians. https://physiciansfoundation.org/research/examining-physician-resident-and-student-wellbeing-and-impact-of-the-current-healthcare-landscape/
[8] Westbrook JI, Raban MZ, Walter SR, Douglas H. Task errors by emergency physicians are associated with interruptions, multitasking, fatigue and working memory capacity: a prospective, direct observation study. BMJ Qual Saf. 2018;27(8):655-663. doi:10.1136/bmjqs-2017-007333. https://pubmed.ncbi.nlm.nih.gov/29317463/
[9] Agency for Healthcare Research and Quality Patient Safety Network. A systematic review of the psychological literature on interruption and its patient safety implications. https://psnet.ahrq.gov/issue/systematic-review-psychological-literature-interruption-and-its-patient-safety-implications