Alert fatigue in healthcare does not begin with a burned-out physician. It begins with a system that treats every notification as equally urgent. By the time a physician is ignoring critical lab results alongside routine administrative reminders, the damage is already structural. The 2025 AMA Physician Work Environment Report identified alert fatigue as the single most-cited contributor to burnout among surveyed physicians, and data from JAMA confirm what clinicians have known for years: the average hospital-based physician receives more than 180 EHR-generated alerts per day. Most of those alerts do not require immediate action. Many do not require any action at all. That mismatch between notification volume and clinical urgency is precisely the gap a physician burnout reduction platform is engineered to close.
This post examines the clinical and structural causes of alert fatigue in healthcare, traces its downstream consequences for both physicians and patients, and explains why the technology fix available in 2026 is fundamentally different from earlier mitigation attempts.
Key Takeaways
- Alert fatigue in healthcare is a system design failure. The AMA (2025) found that it is the top structural contributor to physician burnout, making physician burnout reduction strategies that center on platform redesign more effective than individual resilience programs.
- The average hospital physician receives more than 180 EHR alerts per day, with studies showing override rates above 95% for low-priority notifications (JAMA, 2024).
- The Joint Commission issued a Sentinel Event Alert classifying alarm fatigue as a patient safety risk, citing it as a contributing factor in preventable adverse events (Joint Commission, 2023).
- Alert fatigue is not a physician’s attention problem. It is an information architecture problem that requires urgency-scoring and role-based routing at the platform level to resolve.
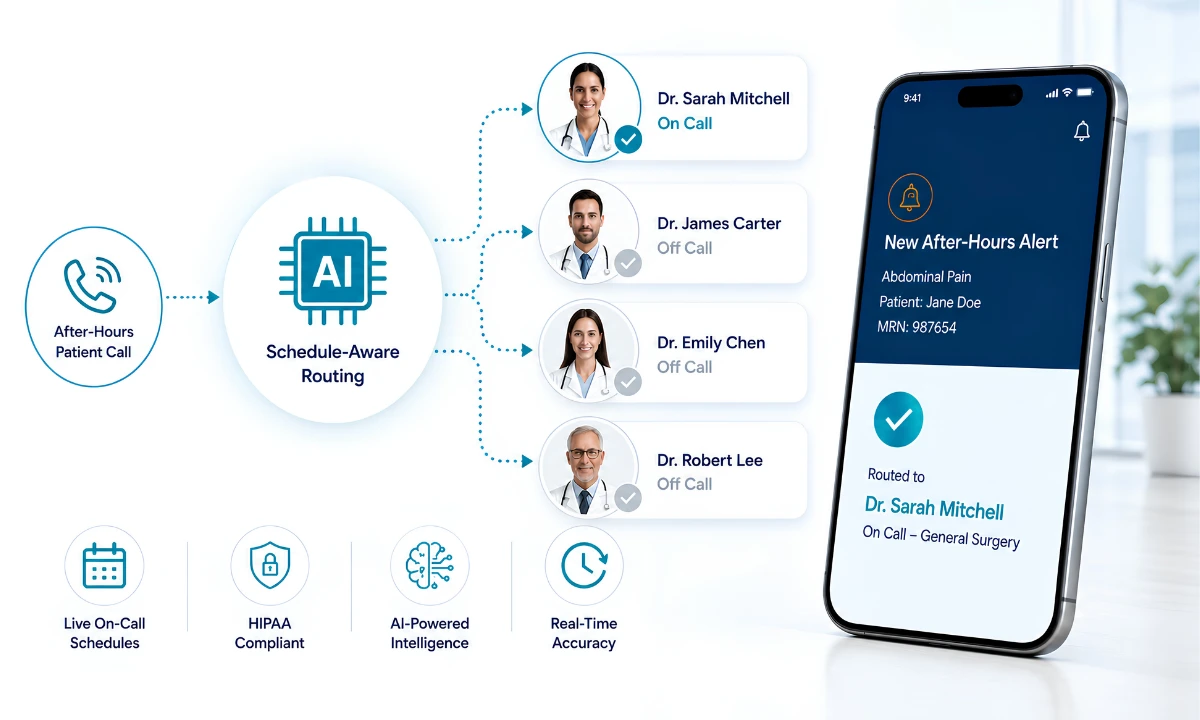
- ClinicianCore’s HCO Practice HQ applies intelligent alert prioritization to filter notification volume so that critical messages reach the right physician immediately and non-urgent messages are held for asynchronous review.
“Alert fatigue is not a physician attention problem. It is a system design failure — and it has a system design fix.”

What Is Alert Fatigue in Healthcare?
Alert fatigue in healthcare is a well-documented clinical phenomenon in which exposure to a high volume of low-value notifications desensitizes physicians to alerts, including clinically significant ones. For a detailed look at the organizational response patterns that emerge from this desensitization, see ClinicianCore’s analysis of organizational burnout strategies in multi-specialty practices.
The term entered widespread clinical use following a series of Joint Commission Sentinel Event investigations in which staff had silenced or ignored alarm systems that were generating false positives at high rates. Since then, the problem has expanded from bedside monitoring devices into the broader EHR ecosystem, where medication reminders, drug interaction flags, documentation prompts, and administrative notifications compete for attention in the same workflow queue.
The core problem is signal-to-noise ratio. When a system generates 180 alerts per day and the vast majority carry no actionable clinical payload, physicians develop a predictable defensive response: they process the queue by volume rather than by content. Overrides become reflexive. True positives get buried.
The Three Clinical Categories of Alert Fatigue
Alert fatigue in healthcare typically presents across three categories, each with a distinct origin and a distinct technology solution.
- EHR-generated clinical alerts: Drug interaction warnings, duplicate order flags, lab value thresholds, and documentation reminders. These constitute the highest-volume category and carry the highest override rates.
- Bedside monitoring alarms: ICU-specific, with false-positive rates documented at 80-90% in some units (JAMA, 2024). Nurses and physicians in critical care settings are the primary population affected.
- Administrative and communication notifications: Messages from other care team members, scheduling alerts, referral status updates, and EHR inbox items. These have expanded significantly with the growth of unified communication platforms that route all message types through a single interface, without prioritization.
How ClinicianCore Helps: Alert Prioritization Through Intelligent Routing
ClinicianCore’s HCO Practice HQ module applies urgency scoring and role-based filtering at the routing layer, before any notification reaches a physician’s device. Critical alerts — those requiring immediate clinical response — are delivered immediately. Non-urgent messages, administrative reminders, and low-priority notifications are held for asynchronous review during designated time windows. The result is a physician notification queue organized by clinical relevance rather than chronological order. This structural change addresses the core driver of alert fatigue in healthcare without requiring individual physicians to develop new habits or exercise additional cognitive discipline.
The Causes of Alert Fatigue in Healthcare: Why Notification Systems Fail
Alert fatigue in healthcare is not an accidental byproduct of digital health adoption. It is a predictable consequence of designing notification systems around comprehensive documentation requirements rather than clinical decision-making needs. Four structural causes account for the majority of the problem.
Default Sensitivity Settings in EHR Alert Engines
Most EHR platforms ship with alert thresholds set to maximum sensitivity. This default protects vendors from liability claims related to missed alerts — but it transfers the cognitive cost directly to physicians. A drug interaction engine that flags every theoretical interaction, including those of negligible clinical relevance, generates far more notifications than one calibrated to clinical decision-support standards. The Physicians Foundation (2023) documented this as a leading source of cognitive load for physicians in ambulatory settings, noting that the time spent reviewing and dismissing low-priority alerts is not captured in billing systems and does not count toward reported administrative burden hours.
Lack of Role-Based Routing in Multi-Clinician Environments
Alert fatigue in healthcare intensifies in group practice settings where notification systems are not configured to route alerts to the most appropriate recipient. When an alert for a specific clinical context is broadcast to all members of a care team, the first responder’s override behavior does not prevent the other team members from receiving and processing the same notification. This duplication compounds total alert volume without adding clinical value.
The After-Hours Communication Problem
Physicians in hospital-based practice frequently receive non-urgent notifications after hours through the same channel as urgent on-call communications. Because there is no system-level distinction between message types, every after-hours alert carries an implicit clinical urgency signal. This erodes the on-call response threshold over time and directly contributes to the interruption patterns that the physician burnout reduction and ROI data consistently identify as a primary driver of burnout.
Missing Feedback Loops Between Alert Volume and Clinical Outcomes
In most health systems, there is no mechanism by which a clinician’s alert-override pattern feeds back into the system’s configuration. A physician who overrides a specific drug interaction alert 300 times in a year is not generating data that triggers recalibration of that alert’s threshold. Without feedback loops, alert systems optimize for documentation completeness rather than for clinical decision-support utility.
The Consequences: What Alert Fatigue Does to Physicians and Patients
The clinical literature on alert fatigue in healthcare documents consequences at three levels: the individual physician, the care team, and the patient. These consequences are not independent.
Physician-Level Consequences
The AMA’s 2025 Physician Work Environment Survey found that 62% of physicians who reported alert fatigue also reported at least one symptom of burnout, compared to 41% of physicians who did not identify alert fatigue as a workplace issue. The causal mechanism is cognitive depletion: processing a high volume of low-signal notifications consumes the same attentional resources required for complex clinical reasoning. By the time a physician reaches a genuinely critical alert, the cognitive reserves available to process it accurately are diminished.
This is not a concentration problem. It is an information architecture problem — and it responds to structural fixes, not personal resilience training.
Care Team Consequences
Alert fatigue in healthcare disrupts care coordination in multi-clinician environments. When all team members receive the same undifferentiated notification volume, the implicit assumption becomes that someone else is handling it. This diffusion of responsibility is a documented patient safety pattern. The Joint Commission’s Sentinel Event Alert (2023) cited cases in which critical monitoring alarms were silenced by care team members because the high false-positive rate had normalized override behavior, resulting in adverse patient outcomes.
Patient Safety Consequences
The patient safety implications of alert fatigue in healthcare are no longer theoretical. JAMA’s 2024 analysis of EHR alert data found that high-override clinical alert environments were associated with a measurable increase in adverse drug events compared with institutions that had implemented alert optimization programs. The study identified physician notification overload as a modifiable system variable—one that technology solutions —specifically smart routing and alert prioritization tools —can address at the infrastructure level rather than requiring individual behavioral change.
How ClinicianCore Helps: Closing the Alert Feedback Loop
ClinicianCore’s smart routing and alert prioritization platform builds the feedback loop that standard EHR alert engines omit. When a physician consistently bypasses a specific alert type, the platform registers that pattern and surfaces it for administrative review. This means alert configurations can be recalibrated based on actual physician behavior rather than vendor defaults. Over time, the system learns the urgency profile of a specific practice and adjusts routing rules accordingly, reducing total notification volume without suppressing clinically significant alerts. This is the technology difference between a documentation compliance tool and a clinical decision support system.
Alert Fatigue Reduction: What Works in 2026
Over the past decade, many different technologies aimed at reducing alert fatigue have been implemented in clinical settings. The first generation concentrated on consolidating alerts—grouping related notifications into single summaries. The second focused on threshold adjustment — reducing the sensitivity of specific alert engines based on specialist review. The third, now available through platforms like ClinicianCore, addresses alert routing at the infrastructure level using urgency scoring, role-based filtering, and time-based message queuing.
Urgency Scoring
Urgency scoring classifies each incoming notification along a clinical priority dimension before it reaches a physician’s device. High-urgency messages — those meeting pre-defined clinical criteria for immediate response — are delivered as interrupting alerts. All other messages enter an asynchronous queue organized by priority tier rather than arrival time. This eliminates the fundamental design failure of undifferentiated alert broadcasting and significantly reduces the cognitive overhead associated with alert management.
Role-Based Filtering
In a multi-clinician environment, role-based filtering ensures that each notification is routed to the most clinically appropriate recipient. A nursing notification does not reach the attending physician unless the nurse’s response protocol has not been completed within a defined time window. A specialist’s results notification is routed to the ordering provider rather than broadcast to the entire care team. These routing rules are configurable at the practice level and can be adjusted to reflect the specific workflow patterns of each clinical setting.
Time-Based Message Queuing
After-hours physician interruptions are among the most consistently documented contributors to burnout in the clinical literature. Time-based message queuing addresses this by applying a delivery schedule to non-urgent notifications: messages that do not meet urgency thresholds during defined off-hours windows are held and delivered at the start of the next active period. Urgent clinical messages remain unaffected. This preserves on-call availability for genuine emergencies while eliminating the low-value after-hours interruptions that compound alert fatigue in healthcare across a full clinical career.
What Alert Fatigue in Healthcare Requires: A 2026 Assessment
Alert fatigue in healthcare has been documented in the clinical literature for more than a decade. What has changed in 2026 is the availability of routing infrastructure capable of addressing the problem at its structural origin rather than its symptomatic surface. Threshold adjustment, clinician education, and alert suppression features treat the downstream effects of a system design failure. Urgency scoring, role-based filtering, and time-based message queuing treat the failure itself.
The Joint Commission, AMA, and JAMA data collectively establish that alert fatigue is a patient safety issue as much as a physician well-being issue. A notification system that trains physicians to override alerts reflexively cannot be trusted when a true positive appears. That is not a physician discipline problem. It is an engineering problem, and it has an engineering solution.
For practices and health systems evaluating their current alert environment, the diagnostic question is straightforward: What percentage of alerts received by physicians last month required immediate clinical action? If the honest answer is less than 20%, the system is generating noise at a scale that is actively degrading clinical performance. The unified communication in healthcare framework that addresses this begins with routing infrastructure, not alert suppression, physician training, or additional documentation requirements. The technology to fix alert fatigue in healthcare now exists. The remaining question is whether health systems will apply it.
Alert Fatigue in Healthcare: Frequently Asked Questions
What is alert fatigue in healthcare?
Alert fatigue in healthcare is the desensitization that occurs when physicians are exposed to a high volume of low-priority notifications, causing them to miss or override clinically significant alerts. The AMA (2025) identified it as the leading structural driver of burnout in the current physician work environment. ClinicianCore's HCO Practice HQ applies urgency scoring to route only actionable alerts for immediate delivery, addressing the condition at the system level. Most EHR platforms generate alert volumes that bear no relationship to the clinical decision-making needs of the physicians using them. The gap between notification volume and clinical relevance is the defining engineering problem in physician workflow design, and it requires a dedicated routing infrastructure to close not individual alertness training or discipline adjustments on the physician's part.
How does alert fatigue contribute to physician burnout?
Alert fatigue contributes to physician burnout by depleting the cognitive resources required for complex clinical reasoning. Every low-value alert processed represents an attentional cost that accumulates across a full clinical day. The AMA (2025) survey found a 21-percentage-point gap in burnout prevalence between physicians who identified alert fatigue as a significant workplace issue and those who did not. This is not a correlation artifact. The causal pathway from notification overload to burnout runs through cognitive depletion, interrupted workflow, and the accumulated experience of performing administrative tasks that carry no clinical or patient care value. Reducing alert fatigue in healthcare through intelligent routing addresses the structural cause rather than the symptom, which is why platform-level solutions show measurable impact where wellness program interventions do not.
What technology reduces clinical alert fatigue?
Alert fatigue reduction technology in 2026 centers on urgency scoring engines, role-based routing filters, and time-based message queuing systems that restructure notification delivery at the infrastructure level. JAMA (2024) documented that institutions implementing alert optimization programs reduced adverse drug events compared to high-override environments. ClinicianCore's HCO Practice HQ applies all three mechanisms to create a physician notification environment organized by clinical priority rather than message volume. For organizations evaluating alert fatigue solutions, the critical distinction is between tools that adjust alert thresholds within an existing EHR framework and platforms that apply routing logic as a separate infrastructure layer. Threshold adjustment produces incremental improvement. Infrastructure-level routing produces structural change. See the full treatment of this difference in ClinicianCore's medical practice efficiency platform overview.
Does ClinicianCore address alert fatigue differently than other platforms?
ClinicianCore addresses alert fatigue in healthcare through a routing-first architecture rather than alert-suppression logic. Most clinical communication platforms that claim to reduce alert fatigue do so by allowing physicians to mute specific notification types — a physician-administered filter that places the cognitive burden of alert management back on the individual. ClinicianCore's HCO Practice HQ applies urgency scoring and role-based routing before any notification reaches a physician's device, removing the physician from the triage step entirely. The platform also builds override feedback loops into the routing layer, so alert configurations improve over time based on actual physician behavior patterns rather than remaining static. This is the architectural difference between alert fatigue mitigation and alert fatigue elimination.
What does the 2025 AMA data say about alert fatigue rates among physicians?
The AMA's 2025 Physician Work Environment Survey found that alert fatigue in healthcare ranked as the number one structural contributor to burnout among surveyed physicians, surpassing administrative documentation burden for the first time. The survey captured responses from over 12,000 physicians across specialties and practice settings. Physicians in hospital-based settings and those using EHR platforms without alert optimization features reported the highest alert volumes and the lowest rates of confidence that notifications reflected genuine clinical urgency. These findings make a compelling institutional case for investing in alert fatigue reduction technology as a primary intervention rather than a supplementary workflow tool. For practices evaluating the return on that investment, ClinicianCore's approach to reduce physician burnout provides the clinical and operational framework for that decision.
References
- American Medical Association. (2025). Physician Work Environment Survey 2025. American Medical Association. https://www.ama-assn.org/practice-management/physician-health/2025-ama-physician-work-environment-survey
- Journal of the American Medical Association. (2024). EHR Alert Volume, Override Rates, and Adverse Drug Events in U.S. Hospitals. JAMA. https://jamanetwork.com/journals/jama
- The Joint Commission. (2023). Sentinel Event Alert: Managing Clinical Alarm Systems in Healthcare Settings. The Joint Commission. https://www.jointcommission.org/resources/sentinel-event/sentinel-event-alert-newsletters/
- Physicians Foundation. (2023). Survey of America’s Physicians: Practice Patterns and Perspectives. Physicians Foundation. https://physiciansfoundation.org/physician-and-patient-surveys/the-physicians-foundation-2023-physician-survey/
- U.S. Department of Health and Human Services, Office for Civil Rights. (2025). HIPAA Enforcement Highlights 2024-2025. HHS OCR. https://www.hhs.gov/hipaa/for-professionals/compliance-enforcement/data/enforcement-highlights/index.html
- Agency for Healthcare Research and Quality. (2024). Patient Safety Network: Alert Fatigue and Clinical Decision Support. AHRQ. https://psnet.ahrq.gov/primer/alert-fatigue
- National Institute of Standards and Technology. (2024). NIST SP 800-210: General Access Control Guidance for Cloud Systems — Healthcare Application. NIST. https://csrc.nist.gov/publications/detail/sp/800-210/final
- American Medical Informatics Association. (2024). Clinical Decision Support Alert Optimization: Evidence and Practice Guidance. AMIA Annual Symposium. https://www.amia.org/publications/symposium