Every morning in an independent physician practice, the coordination work begins before the first exam room door opens. A routing slip sits at the front desk waiting for a response. The billing team needs a physician’s signature on an authorization form. The lab is holding a result that nursing has not yet received. A referral request occupies an inbox that no one checks until after lunch.
None of this is dramatic. None of it triggers an alert or generates a sentinel event report. It simply costs time: time that physicians spend navigating channels that were never designed to work together.
I spent years in surgical practice watching how fragmented intra-office communication functions as invisible overhead, an operational drag that accumulates quietly across the workday. The front desk runs on phone calls. Nursing uses one messaging thread. Billing works through paper or a separate portal. Physicians are expected to synthesize information arriving from multiple directions simultaneously, often between patients.
The result is not a crisis. It is a tax, imposed daily, measured in minutes, and visible only when you calculate what those minutes cost across a full clinical year.
Key Takeaways
- Physicians spend fewer than half their working hours on direct patient care, per 2024 AMA data; the balance is consumed by indirect care and administrative tasks.
- Intra-office coordination spans at least five distinct roles and three or more disconnected communication channels in a typical independent group practice.
- The Joint Commission reports that communication failures remain a leading cause of harmful clinical errors, with an estimated 67% of communication errors tied to information handoffs.
- Unified intra-office communication reduces the context-switching cost that accumulates when physicians manage fragmented tools throughout the clinical day.
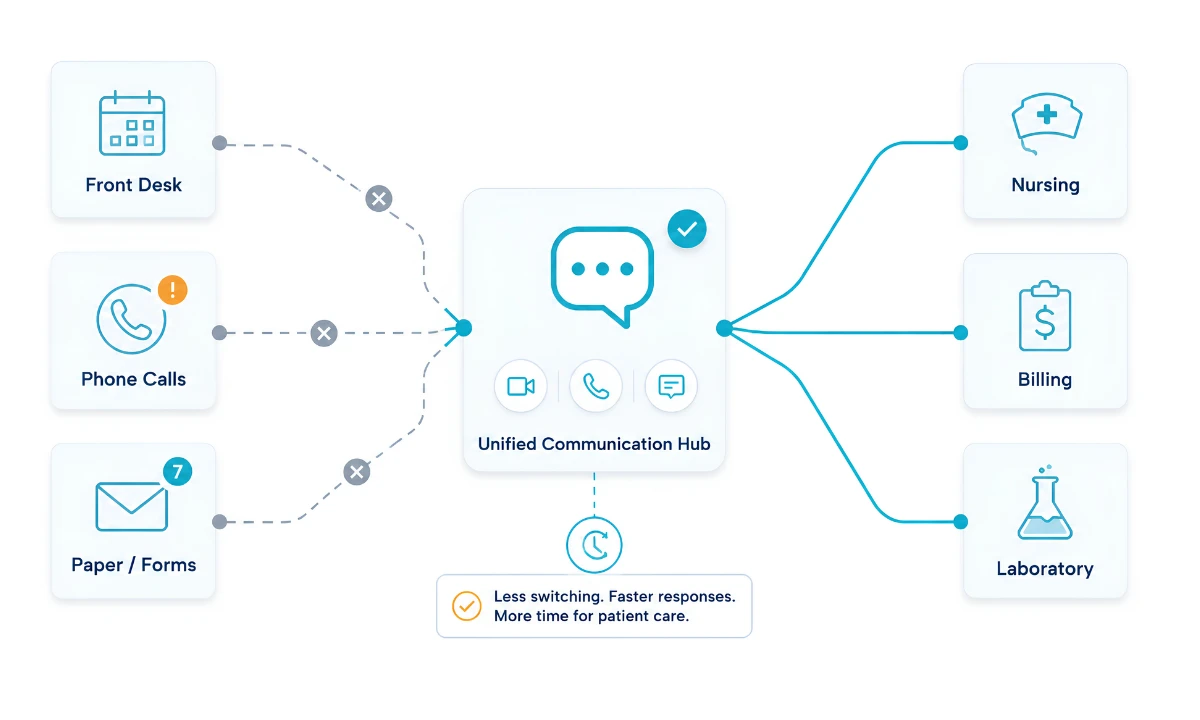
- HCO Practice HQ connects front desk, nursing, physicians, billing, and labs inside a single, role-aware, HIPAA-compliant coordination environment.
“The operating room demands a communication standard that most outpatient practices never apply to their own coordination infrastructure. Messages must reach the right person, at the right time, in the right context. In outpatient practice, this standard rarely exists for the routine operational traffic that governs a physician’s day.”

The Fragmentation Reality in Independent Practices
Independent physician group practices build their internal communication infrastructure incrementally, layering tools as needs arise. A phone system was installed first. An EHR was added. Secure text messaging arrived later. A patient portal introduced a new inbox. A scheduling platform created its own notification channel. Each addition solved a specific problem in isolation.
Together, these tools created a patchwork of disconnected channels that requires every team member, including the physician, to monitor multiple platforms simultaneously. Research published in the Journal of Medical Internet Research confirms what most clinicians already know from experience: time-motion studies show that clinicians spend up to 50% of their working time communicating with others to coordinate patient care. The communication itself is not the problem. The fragmentation is.
When that coordination time is distributed across five or six separate platforms, each with its own interface, notification logic, and response expectation, the cognitive overhead compounds. For surgeons and proceduralists in outpatient settings, this cost is particularly acute. A physician finishing a procedure cannot simultaneously monitor a routing slip, a direct message in the EHR, a phone notification from the front desk, and a text from nursing, while also preparing for the next case. Something waits. And when something waits in clinical practice, the delay becomes a downstream problem for staff, patients, and throughput alike.
Fragmented communication also erodes trust across departments. When the billing team cannot efficiently reach the clinical team, prior authorizations stall. When nursing cannot confirm a routing preference in real time, patient flow slows. When the front desk operates on a different communication channel than the clinical floor, errors of omission become routine. This is the fragmentation tax: not a single catastrophic failure, but a steady daily drain on time, team alignment, and practice performance.
Quantifying the Daily Time Tax
Numbers help frame the scope. The American Medical Association’s 2024 national physician comparison report, drawn from nearly 18,000 physician responses across 43 states, found that of an average 57.8-hour workweek, physicians devote only 27.2 hours to direct patient care. The remaining hours are allocated to indirect care tasks, including order entry, documentation, test result interpretation, and referrals (13 hours per week), and to administrative functions such as prior authorization and insurance forms (7.3 hours per week).
Embedded within those indirect care and administrative hours is a coordination cost that rarely appears in workforce analyses as a distinct line item: the time spent navigating intra-office communication. Locating a result. Confirming a routing decision. Tracking a response from billing. Waiting for nursing acknowledgment. These micro-interactions, individually brief, aggregate across the clinical day into significant time loss.
The 2024 Physicians Foundation Survey of America’s Current and Future Physicians found that six in 10 physicians and residents report often experiencing burnout, with administrative burden identified as a primary driver. The survey underscores that the problem is not limited to documentation volume; it extends to the operational overhead of managing fragmented practice communication across roles and platforms.
From a medical practice efficiency standpoint, the coordination cost is not simply a quality-of-life issue. It directly affects patient throughput, billing cycle time, and staff retention. A practice that requires physicians and staff to expend meaningful time navigating communication fragmentation is a practice operating below its operational capacity, regardless of clinical quality. For a structured look at how these inefficiencies translate into measurable opportunity, the medical practice efficiency platform outlines the core dimensions of this challenge.
How Does Intra-Office Coordination Break Down Between Departments?
The intra-office coordination problem is not uniform. It manifests differently depending on which departments are involved and which direction the communication needs to flow.
Front desk to physician: Scheduling conflicts, patient communication issues, and authorization requests require physician input throughout the day. In most practices, these arrive via phone call, paper message, or EHR inbox items that accumulate while the physician is in the exam room. There is no priority routing, no urgency differentiation, and no acknowledgment mechanism. The physician emerges from a patient encounter and faces an undifferentiated queue.
Nursing to physician: Clinical questions, medication clarifications, and abnormal result flags require a channel that is both immediate and documentable. Verbal relay introduces error. Paging without context wastes time. Secure messaging through EHR systems, where it exists, adds another inbox to monitor without changing the underlying coordination logic.
Billing to clinical: Prior authorization requests, documentation clarifications, and charge capture issues require bidirectional communication between clinical and administrative staff. In many independent practices, this channel is a phone call, a routing slip, or an email thread that lacks HIPAA-appropriate security and leaves no structured audit trail.
Lab and ancillary to physician: Results routing is one of the most consequential intra-office communication flows and one of the most fragmented. A result flagged as abnormal in the laboratory system may travel through two or three intermediaries before reaching the responsible physician. Each handoff is a potential delay or gap.
The Joint Commission, reporting on communication failures in healthcare in August 2024, noted that an estimated 67% of communication errors relate to handoffs: the transitions of information responsibility from one person to another. In outpatient independent practices, these handoffs occur dozens of times daily, across departments, roles, and platforms, with considerably less structure than their inpatient equivalents. The same principle applies at both care levels: unstructured handoffs produce coordination failures, and coordination failures cost time, accuracy, and in some cases, patient safety.
Why Does Addressing Documentation Alone Fall Short?
The dominant response to physician administrative burden in recent years has focused on documentation: ambient AI scribes, voice-to-text tools, optimized EHR templates. These interventions are genuinely valuable and have demonstrated measurable reductions in after-hours documentation time. But documentation burden and coordination burden are distinct problems.
Reducing the time a physician spends charting a patient encounter does not reduce the time they spend waiting for a routing decision from the front desk, tracking down a lab acknowledgment from nursing, or managing an authorization flag from billing. Those coordination functions live in a different layer of practice operations, one that documentation tools do not touch.
A secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, ClinicianCore is designed to address the coordination burden directly. It does not replace the EHR. It provides the communication infrastructure that the EHR was never designed to deliver: real-time, role-aware, priority-differentiated messaging across all departments in the practice.
The distinction matters because the administrative time problem in independent practice is not single-source. The 13 hours per week physicians spend on indirect care tasks, per the 2024 AMA data, includes a coordination component that documentation tools do not address. Practices that invest only in documentation solutions will still face the daily coordination tax that accumulates when front desk, nursing, billing, and labs cannot communicate with the clinical team through a single, intelligent channel.
What Does Unified Intra-Office Communication Require?
Addressing the intra-office coordination gap requires more than installing a group chat tool. A general-purpose messaging platform does not differentiate clinical urgency from administrative routine. It does not integrate with on-call schedules or role-based routing. It does not provide the audit trail required for HIPAA compliance. And it does not connect naturally to the workflows of every department in a physician practice.
A secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians must do several things simultaneously. It must route messages based on role and urgency, ensuring that a critical lab flag reaches the responsible physician immediately while a scheduling question queues appropriately. It must provide acknowledgment mechanisms so that the sender knows the message was received and actioned. It must connect front desk, nursing, clinical, billing, and lab functions inside a single secure environment, eliminating the need for staff to manage parallel channels.
HCO Practice HQ, the organizational communication module of ClinicianCore, which is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, addresses this coordination layer directly. Feature 5 of the platform focuses specifically on intra-office coordination: connecting all practice departments through intelligent routing that breaks down departmental silos, accelerates throughput, and reduces the administrative delays that accumulate when teams operate on disconnected channels.
For independent physician group practices evaluating their communication infrastructure, the question is not whether fragmentation is costing time. The 2024 AMA data confirms that it is. The question is how much, and what that cost represents annually across the clinical team. To estimate the efficiency opportunity for your specific practice, the ClinicianCore ROI calculator provides a structured model based on practice size and communication volume.
The Medical Practice Efficiency Imperative
Medical practice efficiency is not an abstract goal. It is the difference between a practice that runs at the pace the schedule demands and one that absorbs daily friction from coordination failures across departments. The communication fragmentation problem is solvable. It is not a clinical competency issue. It is not a staffing issue. It is an infrastructure problem: a practice operating on a collection of disconnected tools that were never designed to work together, serving a team that cannot afford to spend cognitive bandwidth managing the tools instead of serving patients.
A secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians provides the infrastructure layer that independent practices currently lack. It does not add complexity. It reduces it. When every department routes through the same intelligent channel, physicians stop spending time managing communication logistics and return that time to clinical work.
The Joint Commission’s consistent finding that communication failures remain a leading cause of harmful clinical errors underscores the patient safety dimension of this problem. For the independent physician practice, the efficiency case is equally compelling: fragmented channels cost time, and time is the resource independent practices can least afford to lose. Explore the full operational framework at the medical practice efficiency solutions page.
Frequently Asked Questions
What is intra-office communication fragmentation in a physician practice?
Intra-office communication fragmentation occurs when physicians operate multiple disconnected channels simultaneously, such as phone, EHR messaging, paging, and email, without unified routing or priority differentiation. Each department uses a separate tool, forcing physicians and staff to monitor parallel platforms. This creates coordination delays that accumulate as daily time loss across the clinical team.
How much time do physicians lose to communication and administrative tasks each week?
According to the American Medical Association’s 2024 national comparison data, physicians work an average of 57.8 hours per week, with only 27.2 hours devoted to direct patient care. The remaining hours include 13 hours on indirect care and 7.3 hours on administrative tasks, with intra-office coordination embedded across both categories.
Why does using multiple communication channels increase physician burnout risk?
Managing multiple communication channels simultaneously increases cognitive load and context-switching frequency, two factors directly linked to burnout in clinical settings. The Physicians Foundation 2024 survey found that six in 10 physicians and residents often experience burnout, with administrative burden identified as a primary driver. Fragmented tools add coordination overhead without adding clinical value.
How does unified intra-office communication improve medical practice efficiency?
Unified intra-office communication improves practice efficiency by eliminating the coordination lag that occurs when departments operate on separate channels. Front desk, nursing, billing, and lab can communicate with the clinical team through a single structured platform, reducing delays in routing decisions, authorization processing, and result acknowledgment that otherwise accumulate across the workday.
What intra-office coordination features does HCO Practice HQ provide?
HCO Practice HQ, the organizational communication module within ClinicianCore, connects front desk, nursing, physicians, billing, and lab departments through intelligent role-based routing and HIPAA-compliant messaging. Feature 5 addresses intra-office coordination specifically, breaking departmental silos, accelerating throughput, and reducing administrative delays without requiring staff to manage multiple communication platforms.
References
1. American Medical Association. Doctors work fewer hours, but the EHR still follows them home. AMA Organizational Biopsy 2024 national comparison data. Published August 2025. Available at: https://www.ama-assn.org/practice-management/physician-health/doctors-work-fewer-hours-ehr-still-follows-them-home
2. American Medical Association. Strong care teams are key to boosting physician well-being. AMA 2024 National Physician Comparison Report. Published September 2025. Available at: https://www.ama-assn.org/practice-management/physician-health/strong-care-teams-are-key-boosting-physician-well-being
3. The Physicians Foundation. 2024 Survey of America’s Current and Future Physicians. Published September 17, 2024. Available at: https://physiciansfoundation.org/wp-content/uploads/2024-Survey-of-Americas-Current-and-Future-Physicians.pdf
5. American Medical Association. Electronic health record use research. AMA.org. Updated March 2026. Available at: https://www.ama-assn.org/practice-management/digital-health/electronic-health-record-ehr-use-research
7. Kannampallil TG, et al. Characterizing the Patterns of Electronic Health Record-Integrated Secure Messaging Use: Cross-Sectional Study. J Med Internet Res. 2023;25:e48583. doi:10.2196/48583. Available at: https://www.jmir.org/2023/1/e48583
8. Association Between Conversational Multitasking and Clinician Work Behaviors at a Large US Health Care System: Cohort Study. J Med Internet Res. 2025. Available at: https://www.jmir.org/2025/1/e72768




