A FHIR (Fast Healthcare Interoperability Resources) clinical communication platform is no longer a future-oriented concept for physician practices; it is an operational requirement. The 2026 regulatory environment has accelerated a fundamental change in how healthcare executives evaluate clinical technology. Health systems are no longer selecting monolithic all-in-one platforms. They are identifying gaps in their existing infrastructure and sourcing the connective tissue that allows specialized workflows to function at scale.
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, designed to serve exactly that function. Where EHRs provide the record, ClinicianCore provides the communication layer that connects clinical reasoning, interprofessional consultation, multi-channel coordination, and real-time physician intelligence into a single, FHIR-compatible architecture.
This post covers how ClinicianCore presents itself as the Intelligent Bridge between legacy clinical systems and the API-driven workflows mandated by 2026 compliance, and what that means for physician practices, healthcare developers, and medical group executives evaluating their technology roadmap before the September 2026 market window.
Key Takeaways
- In 2026, healthcare executives evaluate clinical technology based on API connectivity rather than feature count. Specialist platforms addressing specific workflow gaps are replacing monolithic all-in-one systems.
- CMS-0057-F mandates that standard prior authorization decisions be made within 72 hours and urgent decisions within 24 hours, setting a documentation speed requirement that most EHRs cannot meet independently.
- According to the AMA (2024), prior authorization alone consumes an average of 13 hours of physician and staff time per week, with practices completing 39 prior authorizations per physician weekly.
- ClinicianCore’s HCC Consult Core module records each interprofessional consultation as an API-exportable, CPT-coded clinical record, turning informal consultations into compliant, billable events.
- Physician practices that implement FHIR-compatible communication infrastructure before the September 2026 market window will gain a structural advantage over those that respond reactively to compliance requirements
- For the complete strategic framework, refer to the unified clinical communication platform overview.
“By 2026, healthcare executives no longer ask what a platform does; they ask what it connects to. ClinicianCore addresses this new priority by serving as the communication layer that turns every physician consultation into a documented, billable, compliance-ready event.”

Why 2026 Marks an API Inflection Point for Healthcare Technology Decisions
The shift that defined 2025 and 2026 in healthcare technology procurement is architectural. Health system evaluators are no longer asking “what does this platform do?” They are asking, “What does this platform connect to?”
According to HIMSS (2024), integrating data from multiple EHR systems is the most significant obstacle to interoperability, cited by 42% of health systems, a finding that directly reflects the gap that FHIR-native platforms are positioned to fill.
Health systems send an unambiguous message: the era of the monolithic EHR as the sole technology platform is ending. They now use a layered architecture in which the EHR stores the record, while purpose-built platforms handle specialized workflows.
For physician communication, that specialized platform has to do three things simultaneously. It must be HIPAA-compliant at the infrastructure level, not as a feature. It must connect physician-to-physician clinical reasoning to the documentation systems that produce billable, legally defensible records. And it must surface intelligence from across a practice’s data environment to the right physician at the right moment.
ClinicianCore is one of the few unified clinical communication platforms designed for physicians that securely bridge the gap between EHR data and the real-time, actionable clinical dialogue doctors need to deliver care.
What Is CMS-0057-F and Why Does It Create a Clinical Communication Gap?
The Interoperability and Prior Authorization Final Rule (CMS-0057-F) requires payers to return standard prior authorization decisions within 72 hours and urgent ones within 24 hours, setting strict communication timelines for providers.
Those timelines are not just a payer compliance issue. They are a physician communication problem.
Most prior authorization denials that require clinical appeal depend on interdisciplinary reasoning that is currently undocumented: a hospitalist calling a cardiologist for a curbside opinion, a surgeon speaking with a pharmacist to clarify a drug interaction, or a primary care physician discussing a specialist referral. None of that reasoning enters the authorization record. None of it is captured as a clinical document. None of it is exportable to the billing or appeals systems, where it would be most valuable.
According to the AMA (2024), 93% of physicians report that prior authorization causes delays in patient care, and 82% report that patients have abandoned recommended treatment because the documentation process was not completed in time, not because the clinical justification was absent.
ClinicianCore’s HealthCare Collaboration module addresses this gap at the source. HCC documents every interprofessional consultation as a structured clinical record, assigns the appropriate CPT code from the active interprofessional consult series (99446, 99449, or 99451), and makes that record exportable via API to connected billing and appeals systems. For physician practices facing CMS-0057-F compliance timelines, this is not a convenience feature. It is the infrastructure that enables the 24-hour response window.
For a complete breakdown of the mandate’s operational requirements and why EHR architecture cannot meet the 24-hour window, see the dedicated analysis of what CMS 0062-P requires and why existing EHR workflows fall short.
How Does ClinicianCore Function as an Intelligent Bridge in FHIR-Based Workflows?
The phrase “Intelligent Bridge” describes a specific role. It is a platform that connects the EHR and billing system to the physician communication layer, without replacing them. This is where clinical decisions occur.
ClinicianCore uses HL7 FHIR Release 4.0.1 and SMART on FHIR. Third-party AI apps, diagnostic tools, and decision-support agents connect directly to ClinicianCore through a documented, compliant API. A developer building routing, diagnostic, or risk tools bypasses the EHR’s restricted architecture and connects to ClinicianCore’s FHIR-native API, where data is already structured, compliant, and attributable.
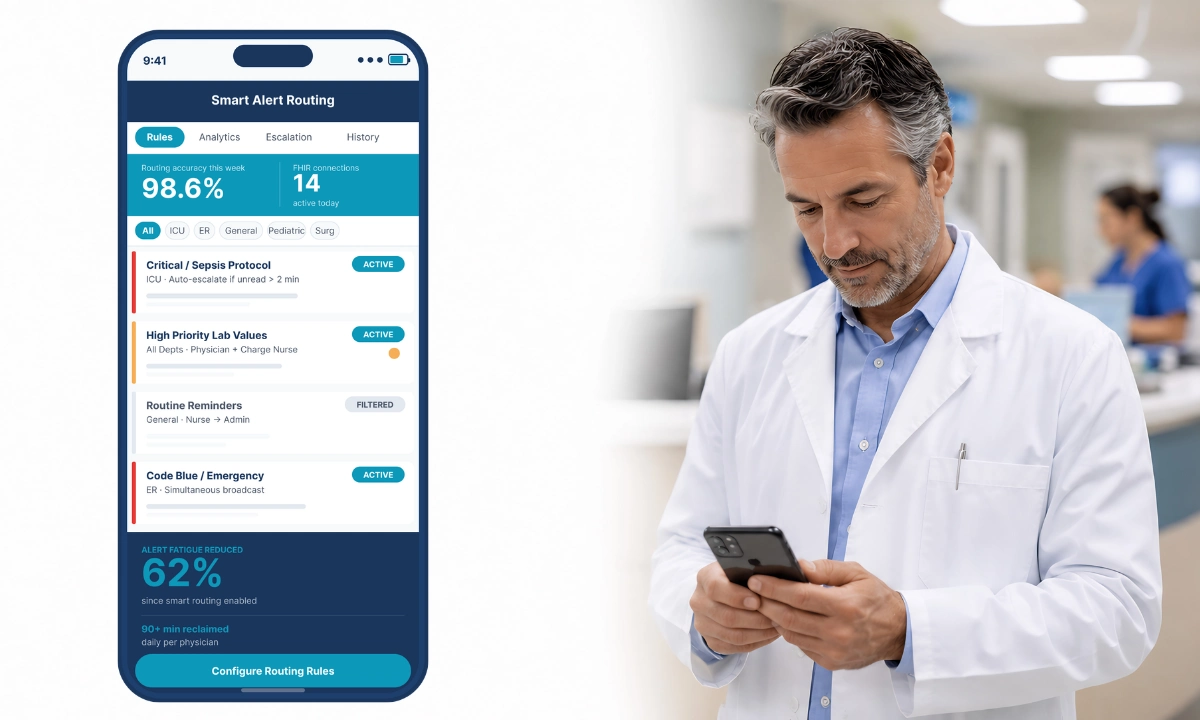
This is critical in three practical scenarios. First, ePA workflows: When prior authorization requires a clinical appeal, the HCC-documented consultation serves as the evidence. It is structured, timestamped, signed, and sent directly to the payer’s API. Second, AI deployment: ClinicianCore supports SMART App Launch 2.0.0. AI agents run as background services in the platform. Third, alert consolidation: The HCO Practice HQ uses routing intelligence to target alerts by specialty, schedule, and role.
ClinicianCore is a secure, HIPAA-compliant clinical communication platform for physicians. Its architecture supports all three scenarios from a single compliant infrastructure.
For a detailed view of the healthcare AI and innovation platform framework, see the full solution overview.
The Clinical Revenue Case for HCC Documentation
Adopting FHIR-integrated clinical communication offers substantial and immediate financial benefits for healthcare organizations.
According to the AMA (2024), prior authorization requirements for a single physician consume the equivalent of 13 hours of physician and staff time per week, and more than a third of physicians have hired staff to work exclusively on administrative documentation, which a structured, CPT-coded consultation workflow directly offsets.
CPT codes 99446, 99449, and 99451 are designed to reimburse interprofessional consultations: 99446 and 99449 apply to telephone or internet consultations between practitioners, based on duration, while 99451 covers written reports furnished in response to consultation requests. CMS (2025) confirmed these codes are eligible for reimbursement on the Medicare Physician Fee Schedule, with 99449 reimbursing approximately $71.84 per consultation.
ClinicianCore’s HCO Practice HQ module captures the interprofessional consultation in real time, assigns the appropriate CPT code based on the documented duration and modality, generates a structured clinical record, and exports it via the FHIR API to the practice’s billing system. The audit trail created by HCC also serves as compliant documentation for prior authorization appeals under CMS-0057-F, creating one clinical event that serves two compliance functions simultaneously.
For a quantified view of time and revenue recaptured, see the overview of the medical practice efficiency platform.
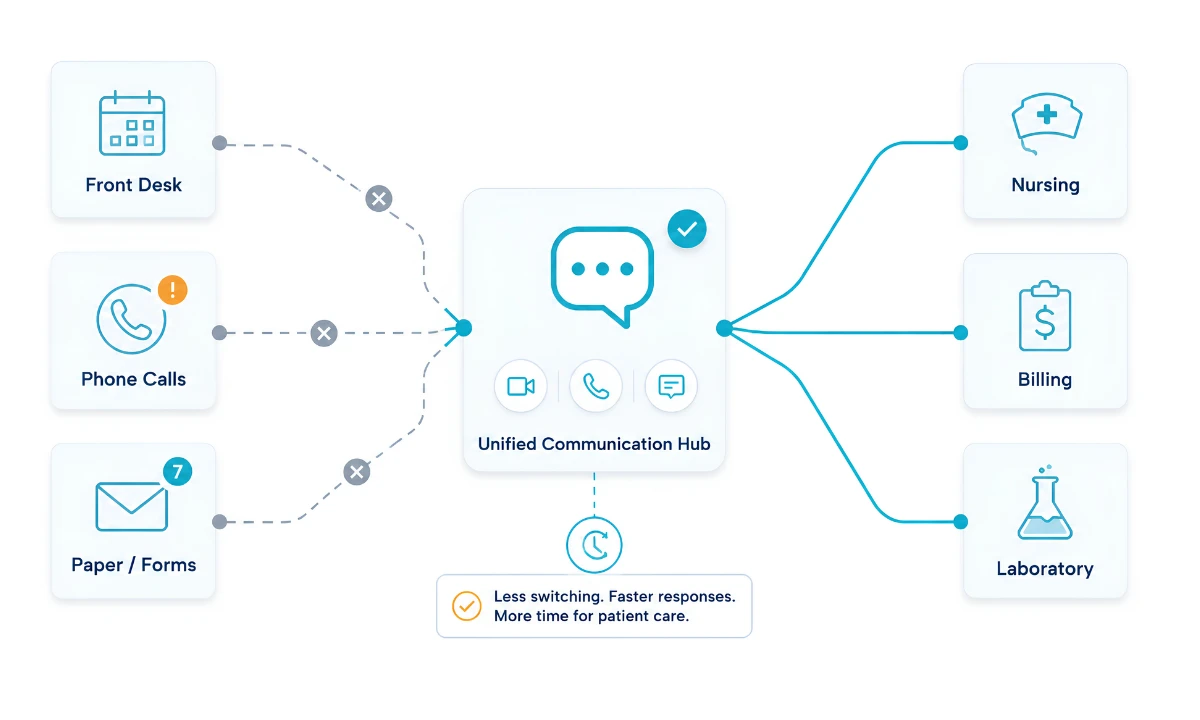
Eliminating Portal Fatigue Across the Multi-Channel Communication Layer
The accumulation of separate AI tools, diagnostic platforms, prior authorization portals, specialty referral systems, and internal notification channels creates an environment where, according to AHRQ (2024), the expansion of non-interoperable health IT applications contributes directly to data fragmentation and information overload, recognized as a threat to the safety, quality, and efficiency of care.
For the routing mechanism behind this consolidation, see how intelligent message routing reduces interruptions for physicians.
The consequence is the opposite of the efficiency these tools were designed to produce. Alert volume increases. Response latency increases. The physician’s cognitive load increases. And accountability for whether any given alert was acted on is distributed across platforms, creating both clinical risk and compliance exposure.
ClinicianCore’s HCX Xchange module helps reduce portal fatigue by giving physicians a single, consolidated view of all their communication, voice, video, and secure messaging. Unlike fragmented systems, it brings together notifications and outputs from third-party AI tools into one unified, prioritized, and secure interface, ensuring clinical information is actionable and easily accessible.
For physician practices, this consolidation directly addresses the portal fatigue metric that most satisfaction surveys now track as a precursor to burnout. See the physician burnout reduction platform for quantified time-savings benchmarks.
ClinicianCore stands apart because it is purpose-built for physicians and clinical workflows. It provides secure, HIPAA-compliant communication tailored to clinical requirements, not adapted from consumer or general business tools. This focus ensures reliability and relevance to frontline physician needs.
Preparing for the September 2026 Market Window
The CMS-0057-F compliance timelines took effect on January 1, 2026, for most covered entities. The proposed CMS 0062-P rule, addressing FHIR-based APIs for drug prior authorization workflows, extends that compliance surface further into 2027. For physician group practices, the strategic implication is clear: practices that proactively establish FHIR-compatible clinical communication infrastructure in the first half of 2026 will gain a lasting competitive advantage over those that respond only to compliance mandates.
The Readiness Gap is not a technology problem for most practices. According to the Physicians Foundation (2024), six in ten physicians and residents reported often experiencing burnout, a figure the survey attributes directly to administrative and operational burdens rather than to clinical workload alone.
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians that connects all three into a single, FHIR-compatible, API-ready deployment. To gain a strategic advantage, act during the September 2026 window by implementing ClinicianCore in your practice. With the included HIPAA-compliant collaboration platform documentation, you receive the compliance evidence package required for organizational procurement approval.
Frequently Asked Questions
What is a FHIR clinical communication platform, and how does it differ from standard messaging tools?
A FHIR clinical communication platform connects physician workflows to HL7 FHIR R4.0.1 APIs, enabling secure data exchange between EHRs, billing systems, and AI applications. Unlike consumer messaging tools, it maintains auditability at every point of exchange. According to the AMA (2024), 82% of physicians report that patients abandon recommended treatment due to prior authorization barriers that begin when clinical reasoning is undocumented at the point of exchange. ClinicianCore closes that gap.
How does ClinicianCore support CMS prior authorization compliance for physician group practices?
ClinicianCore functions as a FHIR-compatible API gateway that routes physician consultation documentation directly into electronic prior authorization workflows, addressing CMS-0057-F timelines of 72 hours for standard requests and 24 hours for urgent requests. According to CMS (2024), documentation lag is the primary barrier to ePA compliance. HCC captures clinical reasoning at the point of consultation.
Can AI agents operate inside ClinicianCore’s communication infrastructure without additional HIPAA compliance setup?
Yes. ClinicianCore supports SMART App Launch 2.0.0, enabling AI agents to operate as background services within the platform’s HIPAA-compliant infrastructure. HCX is fully HIPAA-compliant and serves as a verified environment for deploying agentic AI models on real-world clinical communication data. According to AHRQ (2024), non-interoperable health IT systems directly contribute to data fragmentation and information overload, the primary barriers developers face when deploying AI tools in clinical environments.
How does ClinicianCore’s HCC Consult Core turn interprofessional consultations into billable, documented events?
HCC saves each interprofessional consultation as an organized medical record, linked to special billing codes (99446, 99449, or 99451), which can be sent directly to billing software. The Centers for Medicare & Medicaid Services (CMS) noted in 2024 that many short doctor-to-doctor consults are not recorded, and so doctors are not paid for this time. ClinicianCore makes sure this work is properly recorded and paid.t. Start turning your interprofessional consultations into revenue. Contact us to learn how ClinicianCore can help your practice maximize reimbursements.
What should healthcare executives prioritize in a FHIR-compliant platform for 2026?
Healthcare executives should prioritize three capabilities: FHIR R4.0.1 API compatibility, a signed Business Associate Agreement, and module-level interoperability covering both clinical collaboration and multi-channel communication. According to the AMA (2024), fragmented communication infrastructure ranks among the top operational challenges in physician group practices. ClinicianCore offers immediate access to all three priorities in a unified platform, enabling executives to streamline compliance, safeguard patient data, and facilitate seamless team communication.
References
1. CMS (2024). Interoperability and Prior Authorization Final Rule (CMS-0057-F). Centers for Medicare and Medicaid Services. Retrieved from https://www.cms.gov/regulations-and-guidance/legislation/paperreductionactof1995/pra-listing/cms-0057-f
2. HHS OCR (2024). HIPAA Enforcement Highlights. U.S. Department of Health and Human Services, Office for Civil Rights. Retrieved from https://www.hhs.gov/hipaa/for-professionals/compliance-enforcement/enforcement-highlights/index.html
3. AMA (2024). 2024 AMA Prior Authorization Physician Survey. American Medical Association. Retrieved from https://www.ama-assn.org/system/files/prior-authorization-survey.pdf
4. Physicians Foundation (2024). Survey of America’s Physicians: Practice Patterns and Perspectives. Physicians Foundation. Retrieved from https://physiciansfoundation.org/physician-and-patient-surveys/
5. CMS (2025). Medicare Physician Fee Schedule Final Rule. Centers for Medicare and Medicaid Services. Retrieved from https://www.cms.gov/medicare/payment/fee-schedules/physician
6. AHRQ (2024). Digital Healthcare Research Program: 20 Years of Advancing Innovation and Discovery. Journal of the American Medical Informatics Association. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491618/
7. AHRQ (2023). Patient Safety Network: Health IT Safety and Clinical Communication. Agency for Healthcare Research and Quality. Retrieved from https://psnet.ahrq.gov/primer/health-information-technology-and-patient-safety8. HIMSS / Hyland (2024). Key Takeaways from the HIMSS State of Interoperability Report. Retrieved from https://www.hyland.com/en/resources/articles/5-key-takeaways-himss-report