The healthcare regulatory landscape shifted again in April 2026 with the CMS proposed rule known as CMS 0062 P. The rule extends federal prior authorization reform to drugs and introduces a 24-hour expedited decision window that group practices, outpatient clinics, and community hospitals are not currently equipped to meet.
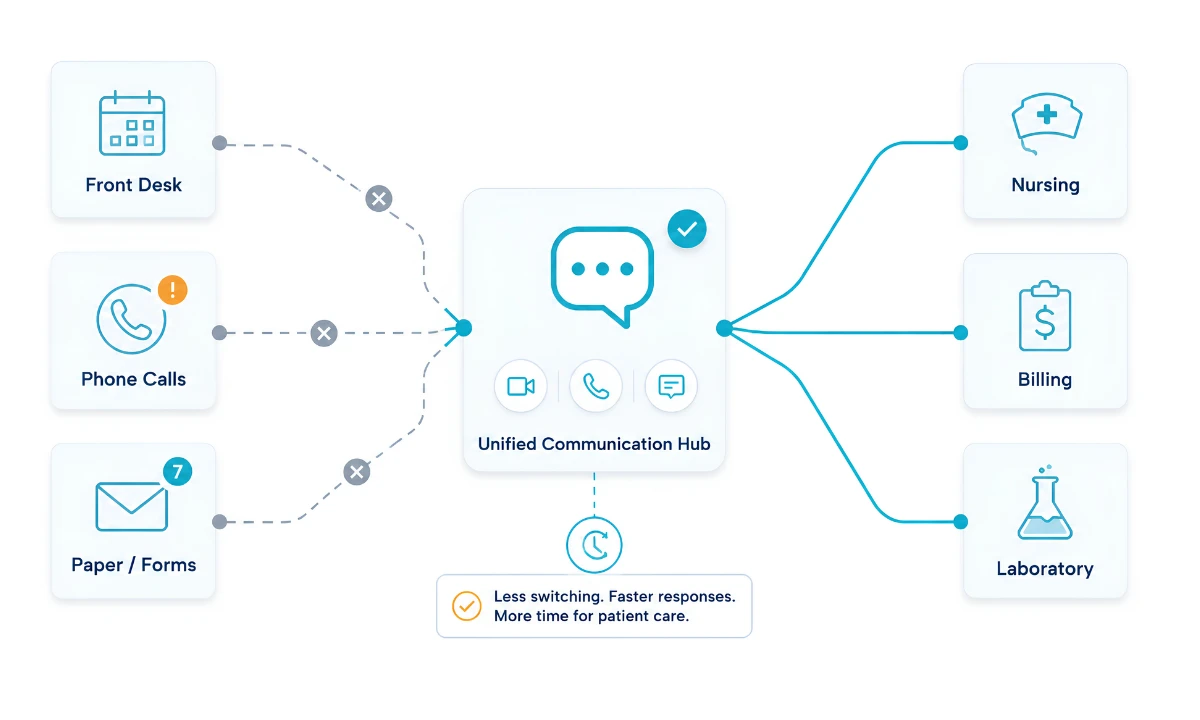
The goal is to focus on patients and prevent treatment abandonment caused by weeklong approval processes. However, the practical challenge is greater. Most Electronic Health Record (EHR) systems are designed primarily for storage and billing, not for quickly sharing clinical evidence among teams. To meet this urgent need, a dedicated high-speed clinical orchestration layer must operate alongside the EHR, not within it.
That layer must also be FHIR-native for a deeper look at the API architecture that makes this possible. See how a FHIR clinical communication platform bridges interoperability beyond the EHR.
ClinicianCore is a HIPAA-compliant unified clinical communication platform designed specifically to address this gap.
Key Takeaways
- CMS 0062 P proposes a 24-hour expedited decision window for drug prior authorization, dramatically tightening the operational tolerance for medical practices.
- Legacy EHRs were architected as documentation systems, not communication systems, and their internal messaging cannot reliably orchestrate multi-role workflows in hours.
- ClinicianCore provides a parallel high-speed lane through four modules: HCO, HCC, HCX, and Doc Lounge
- HCO and HCC together compress the internal and cross-organizational steps of prior authorization into minutes rather than days.
- Beyond compliance, orchestration data exposes throughput bottlenecks and helps reduce physician burnout by removing repetitive coordination work.
What CMS 0062 P Actually Requires
CMS 0062 P builds on the prior authorization momentum established by the 2024 Interoperability and Prior Authorization Final Rule. Where the 2024 rule covered medical items and services across Medicare Advantage, Medicaid, CHIP, and qualified health plans, CMS 0062 P targets the next frontier: drug prior authorization. The headline change is the 24-hour decision window for expedited requests, with standard requests held to a tighter clock as well.
For a group practice, this rewrites the daily workflow. The chart pull, the clinical justification, the specialist sign-off, and the response to a payer query all have to happen inside one calendar day. There is no slack for missed messages, voicemail tag, or staff who are out for the afternoon. Compliance is now a function of how fast the practice can move information between people, not how fast it can type into a system.
CMS 0062 P is a 2026 CMS proposed rule that extends prior authorization reform to drugs and requires payers to issue expedited decisions within 24 hours, forcing medical practices to compress documentation, consultation, and submission workflows into a single business day.
Why Traditional EHRs Cannot Meet the 24-hour Window
EHRs do what they were designed to do. They hold the chart, support orders, and feed the claim. They were never designed to orchestrate a six-person, multi-location decision in real time. Three structural limits show up under the pressure of CMS 0062 P.
Asynchronous by default. EHR inboxes assume a clinician will check them when they next log in. That cadence works for routine results. It does not work when a 24-hour clock is running, and the next reviewer is rounding at a different facility.
Closed to outside organizations. Specialist confirmations, infusion center clearances, and pharmacy benefit manager exchanges typically cross system boundaries. Most EHRs handle this poorly, defaulting to fax, portal logins, or unsecured email.
Documentation first, communication last. When the priority is the legal record, the message thread becomes a side channel. Decisions are made, but the audit trail is fragmented across phone notes, sticky notes, and free-text fields.
The result is the pattern every administrator knows: a prior authorization that technically could have been approved on day one drifts to day five because no single tool was responsible for moving the conversation forward.
Learn more about how a unified clinical communication platform addresses this gap.
The Platforms That Power Clinical Orchestration in ClinicianCore
ClinicianCore approaches CMS 0062 P readiness through four purpose-built modules. Each maps to a distinct phase of the prior authorization lifecycle and to a broader operational priority.
HCO: HealthCare Organization for Internal Coordination
Most prior authorization delays start inside the practice, not outside it. The medical assistant needs a note signed. The biller needs the latest lab. The physician needs a quick yes-or-no. HCO is the secure, HIPAA-aligned space where those exchanges happen in seconds rather than across days. Group practices use HCO to keep front office, nursing, and clinical staff in a single thread tied to a patient case, which is the foundation of medical practice efficiency under a 24-hour clock. See how HCO supports practice efficiency.
HCC: HealthCare Collaboration Across Organizations
Drug authorizations frequently require input from outside the four walls of the practice. An oncologist needs a cardiology clearance. A primary care physician needs a specialist note before a biologic is shipped. HCC is the AI-assisted layer for these cross-organization consults, with structured prompts, embedded documentation, and a path to billable, compliant exchange. HCC is where HIPAA-compliant collaboration stops being a slogan and starts being a workflow. Read more on the HIPAA-compliant collaboration platform.
Doc Lounge: Doctor’s Opinion Count for Peer Support
Faster regulation without faster human support is a burnout accelerator. Doc Lounge is a verified, physician-only space for case review, mentorship, and unstructured peer connections that sustain clinicians under operational pressure. Connected physicians lead better-orchestrated teams, which is why Doc Lounge sits at the center of reducing physician burnout. See the physician burnout reduction platform.
The Business Case for Orchestration Beyond the EHR
CMS 0062 P readiness is a compliance story on the surface and a revenue story underneath. Three financial dynamics matter.
Avoided abandonment. Industry data has consistently linked prior authorization delays to prescription abandonment in the high single-digit to low double-digit range. Hitting the 24-hour window protects fill rates, infusion schedules, and downstream procedural revenue.
Reduced cost to comply. A unified clinical communication platform consolidates the dozen ad hoc tools that medical practices currently glue together. The line-item savings on phones, fax services, secondary messaging apps, and overtime are usually larger than the platform itself.
Visibility into throughput. When prior authorization activity flows through a single orchestration layer, administrators can finally see where time is being lost. Most practices discover that the bottleneck is not where they assumed it would be, and that data drives a continuous reduction in cycle time.
A HIPAA-compliant unified clinical communication platform is also an operational dataset. That dataset is the foundation for healthcare AI and innovation projects that further compress the cycle in the months after CMS 0062 P takes effect.
How to Prepare Your Practice for CMS 0062 P
Practices do not need to wait for the final rule to start preparing. The teams that move first will absorb the change with the least disruption.
- Map the current prior authorization cycle. Document every handoff from intake to payer submission. Note the median and worst-case duration of each step.
- Identify the slowest internal handoff. This is almost always an internal coordination problem rather than a payer problem, and HCO is built to compress it.
- Define cross-organization escalation paths. For each common drug class, list the specialists or facilities whose input is typically required and pre-stage the consult workflow in HCC.
- Set a 24-hour readiness baseline. Pull a representative sample of recent drug prior authorizations and measure how many would have cleared in under 24 hours under current workflows.
- Plan for staff adoption, not just software install. Run short, role-specific onboarding sessions. The platform is only as fast as the slowest user on the case.
The practices that walk into the CMS 0062 P era with these five steps complete will not just be compliant. They will have reset their operating tempo for the next decade of regulatory change.
Frequently Asked Questions
What is CMS 0062 P, and when does it apply?
CMS 0062 P is a 2026 CMS proposed rule extending prior authorization reform to drugs, headlined by a 24-hour expedited decision window for payers. Applicability covers Medicare Advantage, Medicaid, CHIP, and qualified health plan issuers. Effective dates depend on the final rule, but practices should prepare operations now to absorb the shorter cycle.
Why can existing EHRs not meet the 24-hour prior authorization window?
EHRs were designed as documentation and billing systems, not real-time orchestration tools. Their internal messaging is asynchronous, their cross-organization links are weak, and their audit trails are fragmented across notes and free text. Meeting a 24-hour window requires a parallel communication layer purpose-built for multi-role, multi-location coordination.
How does ClinicianCore support CMS 0062 P compliance?
ClinicianCore provides a HIPAA-compliant unified clinical communication platform that orchestrates the people side of prior authorization. HCO accelerates internal coordination, HCC handles cross-organization consults, HCX supports leadership-level rule interpretation, and Doc Lounge sustains physician engagement. Together, the four modules compress documented cycle time well inside the 24-hour mandate.
Does ClinicianCore replace my EHR?
No. ClinicianCore complements the EHR; it does not replace it. The EHR remains the system of record for the chart, orders, and claims. ClinicianCore runs alongside it as the high-speed communication and orchestration layer, capturing the conversations and decisions that traditional EHR inboxes cannot keep up with.
How long does ClinicianCore take to implement?
A typical group practice deployment runs in weeks rather than quarters because ClinicianCore sits alongside the existing EHR rather than replacing it. Most onboarding begins with HCO for internal coordination, adds HCC for cross-organization consults, then layers in HCX and Doc Lounge The speed of value depends on staff adoption and workflow mapping at go-live.
References
- Centers for Medicare and Medicaid Services. CMS 0062 P, Proposed Rule on Prior Authorization for Drugs. CMS.gov, 2026.
https://www.cms.gov/priorities/burden-reduction/overview/interoperability/policies-regulations/cms-interoperability-standards-prior-authorization-drugs-proposed-rule-cms-0062-p - Centers for Medicare and Medicaid Services. CMS 0057 F, Interoperability and Prior Authorization Final Rule. CMS.gov, 2024.
https://www.cms.gov/cms-interoperability-and-prior-authorization-final-rule-cms-0057-f - U.S. Department of Health and Human Services. HIPAA Privacy and Security Rules. HHS.gov.
https://www.hhs.gov/hipaa/for-professionals/privacy/index.html - Office of the National Coordinator for Health IT. Interoperability Standards Advisory. HealthIT.gov. https://www.healthit.gov/isa
- American Medical Association. Prior Authorization Physician Survey. AMA, 2024.
https://www.ama-assn.org/system/files/prior-authorization-survey.pdf - Agency for Healthcare Research and Quality. Care Coordination and Health IT. AHRQ.gov.
https://www.ahrq.gov/ncepcr/research/care-coordination/index.html - Commonwealth Fund. High U.S. Health Care Spending: Where Is It All Going? commonwealthfund.org, 2023. https://www.commonwealthfund.org/publications/issue-briefs/2023/oct/high-us-health-care-spending-where-is-it-all-going
- Healthcare Information and Management Systems Society. Clinical Communication and Collaboration. HIMSS.org. https://www.himss.org/resources/clinical-communication-and-collaboration