Physician on-call burnout is not an attitude problem, a resilience deficit, or an unavoidable consequence of clinical life, least of all after hours. It is a structural communication design failure. The American Medical Association (2025) identifies after-hours communication burden as the single leading driver of physician burnout, surpassing documentation load and administrative overhead. When a physician finishes a grueling twelve-hour shift, and their phone continues to deliver non-urgent messages through the recovery window, the system is not supporting care it is consuming the person delivering it.
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians. Its Health Care Organization (HCO) module approaches on-call burnout as precisely what it is: an engineering problem. The solution is not asking physicians to be more resilient. The solution is building message routing that protects recovery time by design.
This post examines the structural causes of physician on-call burnout, quantifies the patient safety consequences of sleep-disrupted clinicians, and explains how deliberate communication design creates the conditions for genuine recovery.
Key Takeaways
- The AMA (2025) identifies after-hours communication burden as the #1 driver of physician burnout — ahead of documentation, staffing shortages, and administrative overhead.
- JAMA (2024) reports that non-urgent overnight alerts reduce total physician sleep time by an average of 1.3 hours per on-call night, compounding cumulative fatigue across the call schedule.
- The Joint Commission (2023) links physician sleep deprivation directly to elevated clinical error rates, making on-call recovery a patient safety issue, not merely a wellness concern.
- MGMA (2024) found that physicians carrying heavy on-call loads are 2.4 times more likely to report intent to leave their current practice within 24 months.
- ClinicianCore’s HCO on-call scheduling module suppresses non-urgent messages during off-call windows entirely — not silencing notifications, but preventing them from being delivered until the physician is next on-call.
- Physicians seeking structural support for the on-call communication burden can explore the physician burnout reduction platform for a full overview of ClinicianCore’s approach.
What is Physician On-Call Burnout? Defining a Structural Problem
Physician burnout describes a state of chronic occupational stress characterized by emotional exhaustion, depersonalization, and a reduced sense of professional efficacy. On-call burnout is a specific, compounding variant of this state, generated not primarily during clinical hours but during the recovery windows between them.
The defining feature of on-call burnout is involuntary cognitive engagement during designated rest periods. A physician who cannot disengage from clinical communication during off-call hours cannot recover. The Physicians Foundation (2023) found that 63% of surveyed physicians reported difficulty fully disengaging from work during off-call periods, with the majority citing notification-driven interruptions as the primary cause.
This is a communication architecture failure. The message-routing infrastructure for on-call physicians determines whether the off-call window is a genuine recovery period or a diluted continuation of the previous shift. Urgency filtering — the systematic separation of critical escalations from routine notifications — is the structural mechanism that makes recovery possible. Without it, physicians receive the same message type whether the patient is deteriorating or whether a colleague needs a non-urgent callback.
The difference between a structural and a cultural approach to this problem matters clinically. Cultural approaches — resilience training, wellness programs, mindfulness apps — do not change the volume or timing of message delivery. A physician completing a mindfulness module at 2 a.m. while their phone continues to alert is receiving wellness programming without structural protection. Only communication design changes delivery patterns.
How Does After-Hours Communication Burden Drive Physician Fatigue?
After-hours communication burden refers to the cumulative volume, frequency, and cognitive demand of clinical messages received outside scheduled work hours. The AMA (2025) Physician Work Environment Survey identifies this burden as the top driver of burnout across specialties, with surgeons, hospitalists, and primary care physicians reporting the highest exposure.
The mechanism is layered. Annals of Internal Medicine (2024) describes three compounding effects from after-hours communication overload:
- Sleep fragmentation: Even notifications that do not require an active response interrupt sleep architecture, preventing the restorative deep sleep stages that reduce cortisol and support immune function.
- Anticipatory arousal: Physicians who have experienced repeated night alerts report elevated resting alertness even on nights without calls a conditioned state that prevents full sleep even when no messages arrive.
- Cognitive load carryover: Clinically complex messages received overnight require active problem-solving that persists into the following clinical day, reducing the cognitive resources available for patient care.
MGMA (2024) provides an operational correlate: physicians with above-median on-call hours reported a 2.4-fold higher intent to leave their practice within 24 months. The physician retention crisis facing medical practices is not separable from the on-call communication design choices those practices have made or inherited.
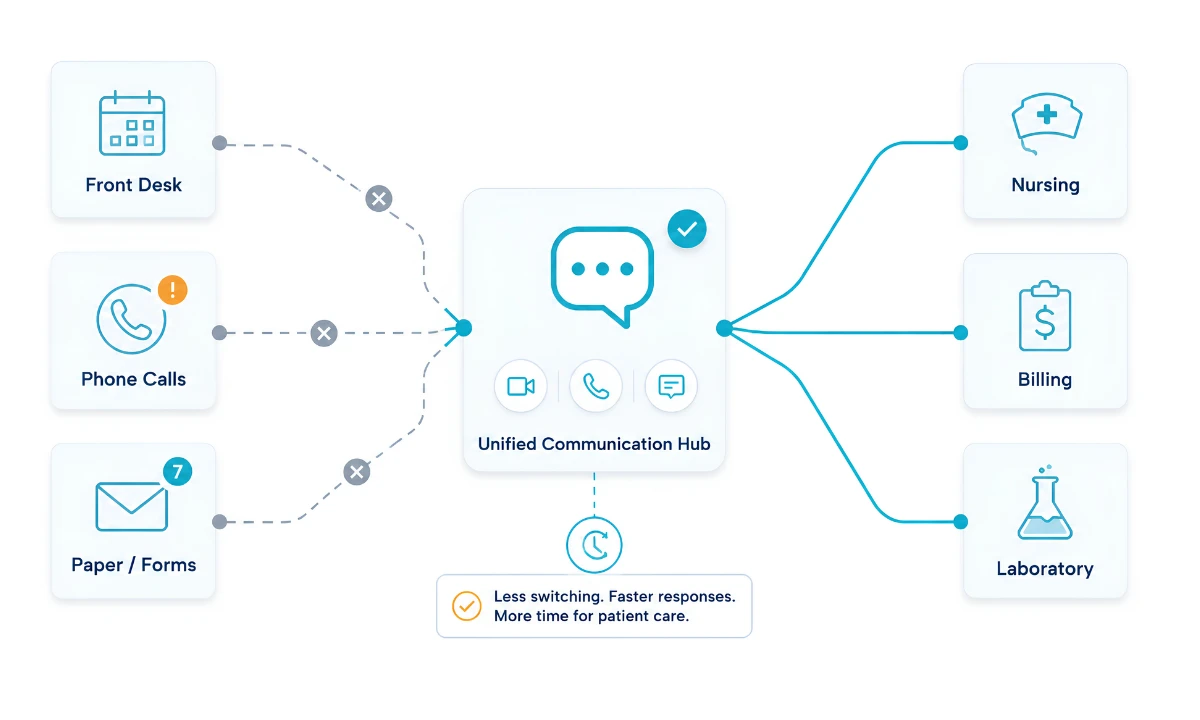
Consumer messaging applications widely used for clinical communication in practices that have not adopted a dedicated platform lack urgency filtering, on-call scheduling integration, and delivery suppression. A message sent via a consumer messaging application arrives whether the receiving physician is in surgery, driving, asleep, or on vacation. Unlike consumer messaging applications, ClinicianCore’s HCO Practice HQ routes messages based on real-time on-call schedule data, suppressing non-urgent delivery when the physician is off-call.
Sleep Disruption and Patient Safety: The Clinical Consequence of Poor On-Call Communication Design
Physician on-call burnout is a patient safety issue — and its after-hours dimension is where patient risk is highest. The Joint Commission (2023) Sentinel Event Alert on fatigue and sleep deprivation establishes a direct causal link between clinician fatigue and elevated clinical error rates, including medication errors, missed diagnoses, and procedural complications.
JAMA (2024) quantifies the impact of non-urgent overnight alerts on sleep. Physicians receiving non-urgent clinical notifications during on-call nights lose an average of 1.3 hours of sleep per call night. Across a monthly call schedule, this deficit compounds to a chronic sleep deprivation state equivalent to the impairment profile studied in alcohol intoxication research.
The safety-design connection is direct. When a healthcare organization chooses to route all clinical messages through a single undifferentiated channel with no overnight suppression logic, it is making a design decision that reduces the cognitive capacity of the physicians caring for its patients the following morning. This is not an abstract wellness concern. It is an organizational liability.
AHRQ (2024) data on adverse events in hospitals identify care transitions and overnight handoffs as the periods with the highest density of adverse events. Fatigued physicians completing overnight on-call coverage are most likely to be involved in these transitions. Improving on-call communication design reduces fatigue precisely where it causes the most harm.
The medical practice efficiency platform at ClinicianCore addresses this risk from an organizational perspective — building the operational systems that allow practices to make structural communication design changes without manual coordination overhead.
What Does Structural Change in On-Call Communication Design Look Like?
Structural change in on-call communication design has three components: urgency classification, schedule integration, and delivery logic. Each must be present for the system to protect recovery time effectively.
1. Urgency Classification
Urgency classification requires the platform to distinguish between message types before routing them. A critical patient deterioration alert, a nursing question about a non-urgent medication refill, and an administrative request for a signature are three different objects. Routing them identically — as most consumer messaging applications and legacy paging systems do — assigns the same urgency weight to all three. This is the root cause of notification overload.
ClinicianCore HCO’s smart routing and alert prioritization engine classifies incoming messages by urgency tier before delivery. Critical alerts penetrate the off-call window. Non-urgent messages enter a delivery queue for the next on-call period. Administrative messages are routed to the appropriate non-physician staff. The physician receives only what genuinely requires their attention during their recovery window.
The smart routing and alert prioritization feature page provides the full technical specification for HCO’s classification logic.
2. Schedule Integration
Urgency classification without schedule awareness is incomplete. A message classified as non-urgent still requires a routing decision: who is on-call to receive it, and when? Without integration between the urgency classification engine and the current on-call schedule, the system cannot route appropriately.
ClinicianCore’s on-call schedule management for physicians module maintains a real-time schedule state. When a physician transitions from on-call to off-call status, the delivery suppression logic activates automatically. No manual do-not-disturb toggle. No physician needs to remember to switch a setting. The schedule drives the routing.
3. Delivery Logic
Delivery logic is the operational expression of urgency classification and schedule integration. For a physician currently off-call, the system must suppress non-urgent deliveries, log the message for retrieval during the next on-call period, and ensure that the covering on-call physician receives time-sensitive items. This requires message persistence, coverage mapping, and escalation pathways.
Traditional paging systems do not provide this delivery logic. A page goes to the pager, regardless of call status. Consumer messaging applications deliver to the device, regardless of whether the physician is available to act. Only a platform with built-in schedule awareness and urgency classification in its routing architecture can execute delivery logic that protects recovery time.
How ClinicianCore HCO Protects Physicians During Off-Call Hours
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians. The HCO Practice HQ was designed specifically to address the structural causes of physician on-call burnout, integrating on-call schedule management and smart routing into a single system rather than configuring them separately.
When a physician enters off-call status in the HCO system, non-urgent messages are suppressed — not merely silenced on the device, but withheld from delivery until the physician is next on-call. Only true critical escalations penetrate the off-call window. This is the communication design change that allows genuine recovery. The phone being quiet is not a matter of willpower or discipline. It is a consequence of how the system routes messages.
This design distinction matters for physician burnout reduction at the organizational level. A practice implementing ClinicianCore HCO is not asking physicians to manage their own boundaries more effectively. It is removing the structural mechanism that was making those boundaries impossible to maintain. Physicians working within a properly configured HCO environment report a different on-call experience — one where recovery is a designed outcome, not a personal achievement.
For practices exploring how after-hours communication redesign fits within a broader physician burnout-reduction platform strategy, ClinicianCore’s solution documentation describes the full integration among HCO scheduling, smart routing, and the physician-facing experience.
Related reading: the post on alert fatigue in healthcare addresses the broader notification overload problem that compounds on-call burnout, and the post on organizational strategies for physician burnout reduction situates on-call communication design within a complete organizational change framework.
The Specific Next Step for Healthcare Organizations
On-call schedule design and message routing architecture are not HR issues. They are clinical infrastructure decisions with direct consequences for physician recovery, retention, and patient safety. The AMA (2025) data is unambiguous: after-hours communication burden is the primary driver of physician burnout. The Joint Commission (2023) is equally direct: fatigue from disrupted sleep elevates clinical error rates.
The specific action available to healthcare organizations is not a new wellness initiative. It is an audit of how clinical messages are classified, routed, and delivered to off-call physicians — and a decision about whether the current architecture is designed to support physician recovery or simply to deliver every message to every physician at every hour.
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, and the HCO Practice HQ exists for exactly this purpose. Schedule-integrated smart routing is not a feature enhancement. It is the structural change that converts the off-call window from an interrupted continuation of clinical work into a genuine recovery period.
Frequently Asked Questions
What causes physician on-call burnout?
Physician on-call burnout is caused primarily by after-hours communication burden, specifically the delivery of non-urgent messages during recovery windows. The AMA (2025) identifies the after-hours communication load as the leading driver of burnout across all specialties. ClinicianCore HCO addresses this cause structurally by suppressing non-urgent message delivery during off-call periods.
How does after-hours communication design affect physician recovery?
After-hours communication design determines whether physicians receive only critical escalations or the full undifferentiated message load during recovery windows. JAMA (2024) found that non-urgent overnight alerts reduce physician sleep by an average of 1.3 hours per on-call night. ClinicianCore’s HCO Practice HQ enforces delivery suppression during off-call status, protecting sleep architecture by design.
Can on-call scheduling software reduce physician burnout?
On-call scheduling software reduces physician burnout when it integrates directly with message routing, not when it only manages shift assignment. The Physicians Foundation (2023) found that physicians with visibility into their structured call schedules reported lower burnout scores. ClinicianCore HCO links the schedule state to delivery logic, so off-call status automatically triggers message suppression without physician action.
What is the difference between on-call fatigue and general physician burnout?
On-call fatigue is an acute, schedule-driven state resulting from disrupted sleep during call-coverage periods. General physician burnout is a chronic occupational syndrome driven by cumulative overload across all domains of clinical work. The Joint Commission (2023) identifies both as patient safety risks, and ClinicianCore HCO addresses on-call fatigue as a recoverable structural problem rather than a fixed occupational condition.
How does ClinicianCore HCO protect physicians during off-call hours?
ClinicianCore HCO protects physicians during off-call hours by integrating real-time schedule data with the smart routing engine, so non-urgent messages are withheld from delivery—not silenced, but held until the physician is next on call. Only critical escalations penetrate the off-call window. ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians.
References
1. AMA (2025). Physician Work Environment Survey. American Medical Association.
2. Physicians Foundation (2023). Survey of America’s Physicians: Practice Patterns and Perspectives.
3. JAMA (2024). Sleep Disruption from Non-Urgent Clinical Alerts and Physician Fatigue. JAMA Network.
5. Joint Commission (2023). Sentinel Event Alert: Fatigue, Sleep Deprivation, and Patient Safety.