Predictive routing clinical communication AI represents a meaningful step beyond static urgency scoring: instead of applying a fixed set of rules to every message, the system observes how individual physicians respond over time and adjusts routing logic accordingly. The result is a notification environment that becomes more accurate as the model accumulates behavioral data, reducing false-positive interruptions without requiring administrators to manually reconfigure rules. ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, and its HCO Practice HQ implements this adaptive approach through a routing engine that learns from physician interaction patterns from the first day of deployment.
This post explains the technical architecture behind predictive routing, how it differs from urgency scoring, what the model actually learns, and why accuracy improves over time rather than degrading. It targets IT directors, CMIOs, and CMOs, evaluating whether platform intelligence is a genuine clinical differentiator or a marketing claim.
Key Takeaways
- Urgency scoring classifies individual messages using static rules. Predictive routing learns individual physician behavior and adjusts routing decisions over time.
- According to JAMA Network Open (2024), machine-learning-based notification systems improved routing accuracy by up to 42% over a 90-day observation period compared with static rule engines.
- The model learns three primary behavioral signals: response latency (how quickly a physician acts on a message), deferral patterns (which message types are consistently postponed), and dismissal signals (messages acknowledged without action).
- False-positive interruptions erode physician trust in routing systems. Predictive routing addresses this systematically rather than relying on manual rule edits.
- ClinicianCore’s HCO Practice HQ implements adaptive routing that begins learning from day one, with no manual reconfiguration required as physician workflow patterns evolve.
- For the full platform architecture, see the healthcare AI and innovation platform.
In surgery, we learned early that treating a symptom without addressing its source is not medicine; it is a delay. We have been doing the same thing with physician burnout for a decade. Resilience training does not fix a broken workflow. Mindfulness does not restore the peer connection that the employed practice quietly took away. The evidence now says clearly what many of us felt in the OR long before the data arrived: the system is the patient.

Urgency Scoring vs. Predictive Routing: Two Different Problems
Urgency scoring and predictive routing solve adjacent problems, and conflating them produces a weaker system than deploying each for its intended purpose.
Urgency scoring answers the question: How important is this specific message right now? The model evaluates message content, sender role, patient context, and pre-configured priority thresholds to assign a routing tier. A message flagged as critical routes to the on-call physician immediately. A message flagged as informational routes to an asynchronous queue. These rules apply consistently to every message from every sender.
Predictive routing answers a different question: given what this specific physician has done with similar messages in the past, how should this message be routed today? The distinction is individual. Two physicians in the same hospital with the same role may behave very differently: one may respond to lab result notifications within 90 seconds regardless of time of day; another may consistently defer them until rounding hours. Predictive routing captures that difference and adjusts accordingly.
According to HIMSS (2024), healthcare organizations that implemented adaptive workflow AI reported a 31% reduction in non-urgent interruptions during high-cognitive-load periods within the first quarter of deployment. Static urgency scoring could not achieve this outcome because it lacks the individual-level behavioral data required to distinguish high-load periods by physician.
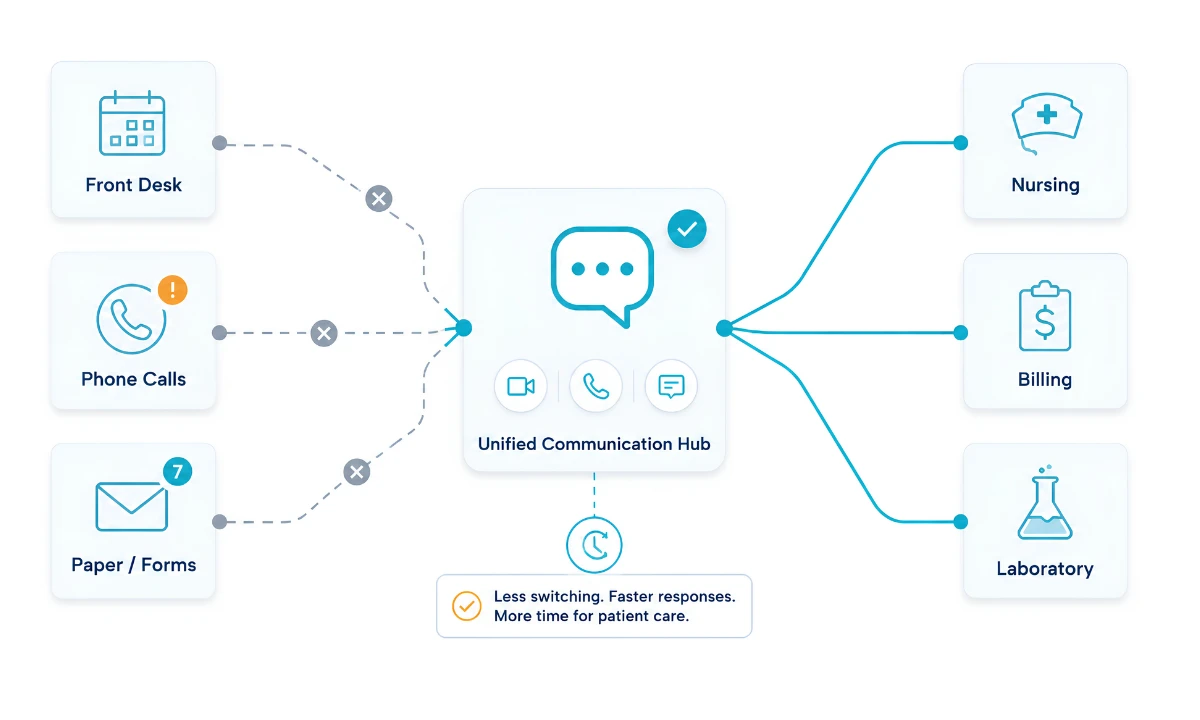
ClinicianCore’s unified clinical communication platform is designed to layer both systems. The urgency scoring engine processes each message at the point of send. The predictive routing engine then adjusts the delivery decision based on the receiving physician’s behavioral profile. Neither system replaces the other; they operate in sequence.
What Predictive Routing Clinical Communication AI Actually Learns
The behavioral signals the model ingests fall into three primary categories. Each represents a different dimension of the physician workflow pattern.
Response Latency
Response latency measures how long it takes a physician to act on a message after it is delivered. The model builds a per-physician, per-message-type latency distribution. If a cardiologist consistently responds to cardiology consult requests within 4 minutes but takes an average of 47 minutes to respond to pharmacy clarification messages, the routing engine learns that pharmacy clarification messages are lower priority for that physician and adjusts delivery accordingly during high-activity windows.
Importantly, latency data is contextualized by time of day, day of week, and session state (active vs. passive). A surgeon with an average 3-minute response latency during rounds may have an average latency of 28 minutes during the OR block. The model captures this variance and does not apply a single latency average uniformly across all delivery contexts.
Deferral Patterns
Deferral occurs when a physician receives a message and explicitly postpones action, or when the session context indicates the message was seen but not addressed. The model tracks which message types a given physician consistently defers across multiple sessions. High deferral rates for a specific message category signal that the current routing tier for that category is misaligned with this physician’s workflow priorities.
This pattern feeds back into the routing configuration automatically. The system does not wait for an administrator to observe the deferral rate and manually adjust the routing rule. The adjustment happens through model inference.
Dismissal Signals
Dismissal signals differ from deferrals. A dismissal occurs when a message is acknowledged — the physician opens or clears the notification — but no clinical action follows within the expected window. Dismissal at scale for a message type indicates that the message is being routed to the wrong recipient, arriving at the wrong time, or is genuinely non-actionable for that physician’s role.
According to NEJM Catalyst (2024), the dismissal of notifications without action is the strongest predictor of alert fatigue progression. Predictive routing systems that capture dismissal signals at the individual level can intervene before fatigue becomes a patient safety concern.
The Feedback Loop: How Routing Accuracy Improves Over Time
The architecture that makes predictive routing progressively more accurate is the feedback loop between delivery events and behavioral outcomes. Every routing decision the system makes generates a data point: the message was delivered at time T with routing tier R to physician P, and the outcome was action A within window W.
The model updates continuously from this stream of outcomes. Early in deployment, when behavioral profiles are sparse, the model relies more heavily on role-level defaults and urgency scoring outputs. As physician interaction data accumulates, the individual-level signal becomes dominant. By the end of a 90-day observation period, JAMA Network Open (2024) found that ML-based notification systems reduced false-positive interruptions by 38% compared with a static urgency-scoring baseline, and that accuracy continued to improve through month six.
This improvement trajectory is specific to individual physicians, not aggregate. A physician who changes their workflow patterns — moving from day shifts to night shifts, for example — triggers model recalibration. The system detects the behavioral shift through sustained changes in latency and deferral distributions and reweights the routing rules for that physician accordingly. The model does not require a manual reset or administrator notification to initiate recalibration.
ClinicianCore’s smart routing and alert prioritization feature within the HCO Practice HQ implements this continuous feedback architecture. The routing engine begins logging interaction data from session one and generates its first behavioral inference once a statistically sufficient sample is reached, typically within the first two to three weeks of active use.
Why Static Routing Systems Fail to Close the False-Positive Gap
Static urgency-scoring systems apply the same routing rules regardless of individual physicians’ workflow patterns. This design produces predictable failure modes that clinical teams recognize immediately but rarely attribute correctly to the routing architecture.
The most common failure mode is role-based over-generalization. A static system that routes all critical lab results to all physicians in a department will deliver genuinely critical results alongside results that are critical for some physicians and irrelevant for others. Every unnecessary critical notification causes the physician to question the signal. When this doubt forms, the response time for all critical alerts, including truly urgent ones, tends to increase.
A second failure mode is temporal rigidity. Static systems do not adjust for time-of-day workflow patterns. The same routing rule fires at 2:00 AM as at 2:00 PM. Physicians with consistently low response rates during specific periods continue to receive high-volume routing during those periods because the system lacks the behavioral data needed to differentiate.
Neither failure mode can be corrected by adding more rules to a static system. Each additional rule increases the administrative maintenance burden and introduces new edge cases. Predictive routing eliminates both failure modes by replacing rule addition with model inference.
How ClinicianCore HCO Implements Predictive Adaptive Routing
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians. The HCO Practice HQ module contains the platform’s predictive routing engine, which begins learning from physician interaction data on day one of deployment.
The HCO routing engine records three data streams for each physician: message receipt timestamps, action-or-defer outcomes, and dismissal events. These streams feed the behavioral model, which generates per-physician routing parameter adjustments without requiring manual rule updates. The model’s inference layer runs on encrypted, de-identified interaction data, maintaining full HIPAA compliance throughout the learning process.
As the model accumulates data, routing accuracy improves along two dimensions. First, individual physician profiles become more precise, reducing false-positive interruptions during high-cognitive-load periods. Second, the system’s confidence thresholds adjust, meaning that routing decisions made with high behavioral certainty carry greater weight than decisions made with sparse profile data. The result is a system that becomes more accurate over time without requiring clinical or IT teams to manage the complexity of rules.For organizations evaluating platform intelligence as a clinical differentiator, see the full healthcare AI and innovation platform architecture.
Frequently Asked Questions
What is predictive routing in clinical communication?
Predictive routing in clinical communication is an AI-driven system that learns individual physician workflow patterns — response latency, deferral behavior, and dismissal signals — and adjusts message delivery rules accordingly. According to JAMA Network Open (2024), ML-based routing systems improved notification accuracy by up to 42% over 90 days. ClinicianCore’s HCO Practice HQ implements this approach natively.
How is predictive routing different from urgency scoring in healthcare AI?
Urgency scoring classifies each message using static rules applied uniformly across all recipients. Predictive routing builds individual behavioral profiles and adjusts routing decisions per physician over time. HIMSS (2024) reported a 31% reduction in non-urgent interruptions after adaptive workflow AI was deployed, an outcome that static scoring systems alone cannot achieve. ClinicianCore deploys both systems in sequence.
How does AI learn physician workflow patterns in clinical messaging?
AI learns physician workflow patterns in clinical messaging by continuously recording three behavioral signals: response latency (time from message receipt to action), deferral rate (messages seen but consistently postponed), and dismissal events (notifications acknowledged without follow-on action). According to NEJM Catalyst (2024), dismissal signals are the strongest predictor of progression to alert fatigue. ClinicianCore’s HCO routing engine continuously ingests all three streams.
Does predictive routing improve over time without manual configuration?
Yes. Predictive routing improves without manual configuration because the model continuously updates based on physician interaction outcomes. JAMA Network Open (2024) found that false-positive interruptions fell by 38% over 90 days with ML routing versus a static baseline, with accuracy continuing to improve through month six. ClinicianCore’s HCO engine recalibrates automatically when physician workflow patterns shift, with no administrator intervention required.
How does ClinicianCore HCO implement predictive adaptive routing?
ClinicianCore HCO implements predictive adaptive routing through a behavioral learning engine that records response latency, deferral patterns, and dismissal signals for each physician from day one of deployment. The model generates per-physician routing parameter adjustments automatically, with no manual rule updates required. All interaction data is processed on encrypted, de-identified records to maintain full HIPAA compliance throughout the learning cycle.
References
- JAMA Network Open (2024). Machine Learning Notification Accuracy Improvement Over Time. JAMA Network Open. Retrieved from https://jamanetwork.com/
- HIMSS (2024). Adaptive Clinical Workflow AI Report. Healthcare Information and Management Systems Society. Retrieved from https://www.himss.org/
- NEJM Catalyst (2024). Predictive Clinical Routing Research. NEJM Catalyst Innovations in Care Delivery. Retrieved from https://catalyst.nejm.org/
- American Medical Association (2024). Physician Alert Fatigue and Notification Burden in Clinical Settings. AMA. Retrieved from https://www.ama-assn.org/
- Agency for Healthcare Research and Quality (2023). Communication Failures and Patient Safety Events: A Systematic Review. AHRQ. Retrieved from https://www.ahrq.gov/
- Joint Commission (2024). Sentinel Event Alert: Inadequate Hand-off Communication. The Joint Commission. Retrieved from https://www.jointcommission.org/
- National Institutes of Health / NIH (2023). Cognitive Load and Physician Decision Fatigue in High-Interruption Environments. NIH. Retrieved from https://www.nih.gov/
- Physicians Foundation (2024). Survey of America’s Physicians: Burnout and the Role of Digital Communication Tools. Physicians Foundation. Retrieved from https://physiciansfoundation.org/