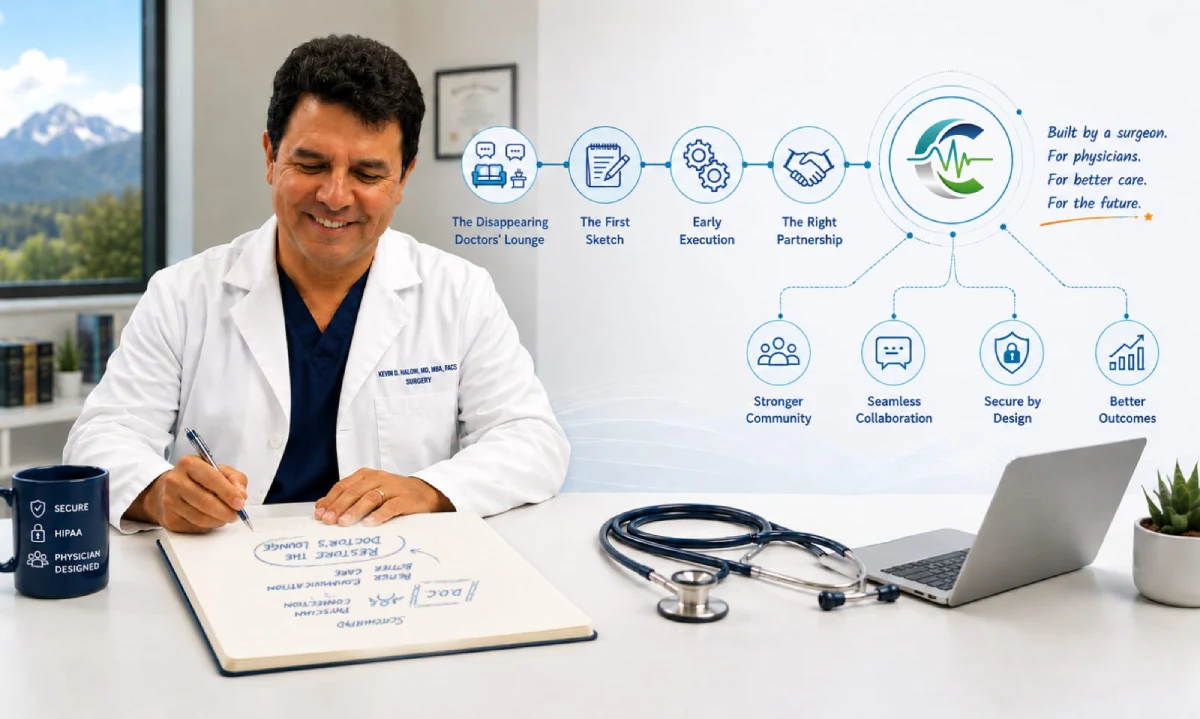
The idea that became ClinicianCore did not start in a venture capital boardroom or a Silicon Valley incubator. It started in a surgery committee meeting when I was the chief of surgery.
For years as a practicing surgeon, I watched the connective tissue of the medical profession dissolve. The formal and informal channels physicians had always relied on to share knowledge, seek a second opinion, and maintain professional community were disappearing, replaced by fragmented digital systems designed for billing compliance rather than clinical thinking.
In surgery, time matters. What you do with the minutes available determines the outcome. I came to see clinical communication the same way; another missed meeting, a misrouted alert, a delayed consultation, or an undocumented hallway question. Each was another clinical value lost, compounding silently into burnout, fragmented care, and a profession increasingly alienated from its own purpose.
ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, exists because the tools available to physicians were not designed by physicians. This is the story of how I chose to change that.
Key Takeaways
- The physical doctors’ lounge, once the informal center of peer learning and clinical support, has largely disappeared from modern medical practice, leaving physicians structurally isolated.
- ClinicianCore began as a physician-only peer community called Doctors’ Opinion Count, wireframed by Dr. Kevin Halow to rebuild lost professional connection in a secure digital environment.
- The platform evolved into a four-module ecosystem, HCO, HCC, HCX, and Doc Lounge, each addressing a distinct communication gap in physician group practices.
- HCO Practice HQ supports documented, billable interprofessional consultations using active 2026 CPT codes 99446 through 99452, converting informal hallway consults into recognized and reimbursable clinical events.
- Every architectural decision was driven by clinical workflow reality, not administrative convenience or technology trends.
“ClinicianCore did not begin as a technology project. It began as an attempt to reconnect physicians to each other. The platform came later. The mission was always the same: restore communication, restore collaboration, and restore the professional community that medicine was built upon.”
 1")
The Disappearing Doctors’ Lounge
There is a place physicians of a certain generation remember vividly: the doctors’ lounge. It was not necessarily glamorous, but it was ours, the physicians. There was a coffee machine running, reasonably comfortable furniture, a television that would find its way to a new channel every time, a refrigerator and bar area with snacks, and breakfast, lunch, and dinner. What happened in that room mattered enormously. There was a vibe in that room. There were informal case reviews and discussions about patients. Peer mentorship passed quietly between generations. Administrators or medical staff leaders would show up to talk to the physicians as they rotated through the revolving doors. It was a time and a place to relax, take a load off, and recharge- emotionally, professionally, and physically.
That room is often gone now. If it is not gone, it has been downgraded. It has been replaced by fragmented digital systems, administrative overhead, and a physical separation between specialties that has become the new norm in medicine. Primary physicians no longer round at the hospital, further enlarging the divide. As this centerpiece of physician engagement disappeared, so did the buffer that helped stem the tide of physician burnout.
According to the Physicians Foundation 2023 Survey of America’s Physicians, 63% of physicians report at least one symptom of burnout. This figure has worsened steadily over the subsequent decade. The American Medical Association has now identified communication dysfunction and administrative burden as primary contributing factors to that trend. When I looked at those numbers, I did not simply see statistics. In it, I recognized many of my colleagues. Most proposals for addressing the physician burnout reduction challenge focused on administrative interventions: EMR optimization, workflow changes, and mindfulness programs, to name a few. None of these addressed the structural void that I saw every day. Physicians had no dedicated, secure space to talk to each other, to get a second opinion at 8 AM or 4 PM, to debate a treatment protocol without someone flagging the thread for compliance review. That observation became a question. That question became a platform.
The First Sketch: Doctors’ Opinion Count (Doc.)
Truth be told, I cannot write a single line of code. If you and I were on a desert island and the only way we could get off was for me to write computer code, we would be in big trouble, with no hope of getting off! I am a surgeon, not a computer programmer. However, a solution to the problem did not require an education in programming language. It turns out that it only required a new look at an old problem.
At that time, I was the Chief of Staff at our 150-bed hospital, and I had just finished my MBA. I was trying to find a way to re-engage physicians by enticing them to attend meetings such as the “Surgery Committee Meeting.” However, instead of using the old “carrot and stick” approach, I changed it entirely. Instead of asking the physicians to go to the meetings, I brought the meetings to them. Using an existing customizable platform, I created a virtual world where physicians could reengage. I began wireframing the communication pathways. I took notes as the hallway and curbside conversations changed. Instead of asking “What happened at the meeting?”, physicians were now commenting and discussing what was on the platform. Over 18 months, I watched as physician engagement grew from 2% to 75%.
The working title captured exactly what I wanted physicians to feel when they used it: Doctors’ Opinion Count. (Doc. for short). The name was a statement of intent. In a healthcare system increasingly organized around billing codes and administrative metrics, the physician’s clinical opinion had been structurally deprioritized; in part because they were so busy taking care of patients that there was no hope for them to engage with each other let alone the medical staff leadership and the administration. I wanted to build a place where the physicians were at the center of the communication, not on the outside, trying to hear it second hand.
The first version was physician-only, verified, and entirely separate from any patient-facing system. As the project grew, an external development team helped me develop a second, more detailed platformed. They translated the wireframes into a live application. The technical path was rough. There were synchronization bugs, stability issues, and server architecture challenges just to name a few examples. On top of all this, I was a one-man band and I was managing this while I was running my surgical practice, seeing patients, operating, and being involved in medical staff leadership. Yet, despite those rough edges, physicians used it with engagement rates similar to the first platform. Soon I added Nurse Practitioners, PAs, Nurses, CRNAs, and administrators. The feedback was good. That validation told me that my underlying premises were correct. It was the answer to a professional loneliness that had gone unnamed for too long.
Early Execution: What No One Tells You About Building in Healthcare
Building healthcare technology while maintaining a clinical practice is not only a challenge of time management. It is an education in consequence management.
In most industries, a bug in your application means a frustrated user. In healthcare communication, a delayed notification, a missed escalation, an unsynchronized message thread carries a weight most software founders never encounter. I have been in operating rooms where seconds determined outcomes. I applied the same threshold of precision to the communication platform I was building.
The early technical failures were exhausting and necessary. Each one clarified exactly what the platform needed to be: reliable before it was rich in features, secure before it was scalable, trusted by clinicians before it was polished for investors. Understand that at this point, it was only an experiment. I was a one-man band wearing all the hats. The purpose of the project was validation only. I wanted to see if it would work.
Thankfully, the hard work paid off. As it turns out, I was on the right track. Interestingly, the Joint Commission has documented “communication failure” as a leading root cause of serious adverse clinical events in U.S. healthcare settings across multiple consecutive reporting periods. However, it was not just the communication issue that I was trying to solve. I was not just building a messaging application. The goal was to close a gap that had genuine clinical consequences when left open. Specifically, physicians were systematically excluded from healthcare decision making, increasingly disengaged from each other and the administration, and burning out in record numbers.
Onboarding hundreds of early physicians and other users by hand, gathering feedback directly, iterating changes in near real time, working with the business school and administrative leaders, all helped me to shape the design even further. The feedback was consistent: physicians wanted a space built for them, not adapted for them.
It was now time to take this to the next level; however, that was something that I could never do alone. Fortunately, that all changed when I met my now partner and CEO, Neeraj Jain.
The Partnership That Expanded the Vision
Taking a project like this from the experimentation phase to a real-world, problem solving, business that could reshape the entire healthcare narrative and place the physicians at the center of HealthCare communication was never in my wheelhouse. I am a surgeon. They don’t teach those sorts of things “Doctor School”. That kind of heavy lift would require someone with expert knowledge and experience in business development. However, it would also require someone who has an intimate knowledge of the actual business of healthcare. It turns out that person was Neeraj Jain.
I met Neeraj Jain on the Y-combinator, a site that was suggested to me by many of my business coaches and mentors. I presented my project on that platform, and I went through hundreds and hundreds of interested individuals until I finally found Neeraj. Neeraj is a healthcare technology entrepreneur with over two decades of experience in Healthcare SaaS and Revenue Cycle Management. Neeraj understood the same fundamental problem I did: clinical healthcare communication in the United States was deeply broken-especially for physicians. However, where I brought clinical context and physician empathy, Neeraj brought strategic architecture, cloud infrastructure expertise, and a precise understanding of how artificial intelligence could optimize clinical communication workflows at enterprise scale.
Neeraj and I represented a synergy in this project that few startups ever obtain. Our partnership was built on complementary expertise. My clinical lens shaped what the platform needed to do for the physician at the point of care. Neeraj’s infrastructure lens shaped how the platform could do it reliably, securely, and at the scale of enterprise health systems. Neither of us was building the same product. We were working together to build different parts of the same solution.
Our union marked the formal beginning of ClinicianCore, and the moment Doc. grew from a single peer community module into a unified four-module clinical communication ecosystem.
What ClinicianCore Became
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, serving physician group practices, outpatient clinics, and smaller community hospitals. Every architectural decision traces back to the original problem: physicians need communication infrastructure that understands clinical workflow, not administrative workflow. Physicians must be at the center of HealthCare communication in order for the business of HealthCare to do its job; provide the highest quality of patient care at the best possible value.
The platform is organized around four distinct communication contexts, each addressing a specific gap identified through personal clinical experience or direct physician feedback that we achieved during the research years of the Doc. early access project. None of the four modules was designed for billing convenience, regulatory reporting, or institutional oversight. Each was designed for the physician delivering care. Each was designed to work both individually and in concert with the other sections in order to put physicians at the center of the Healthcare communication hub.
The Four Modules
HCO: HealthCare Organization
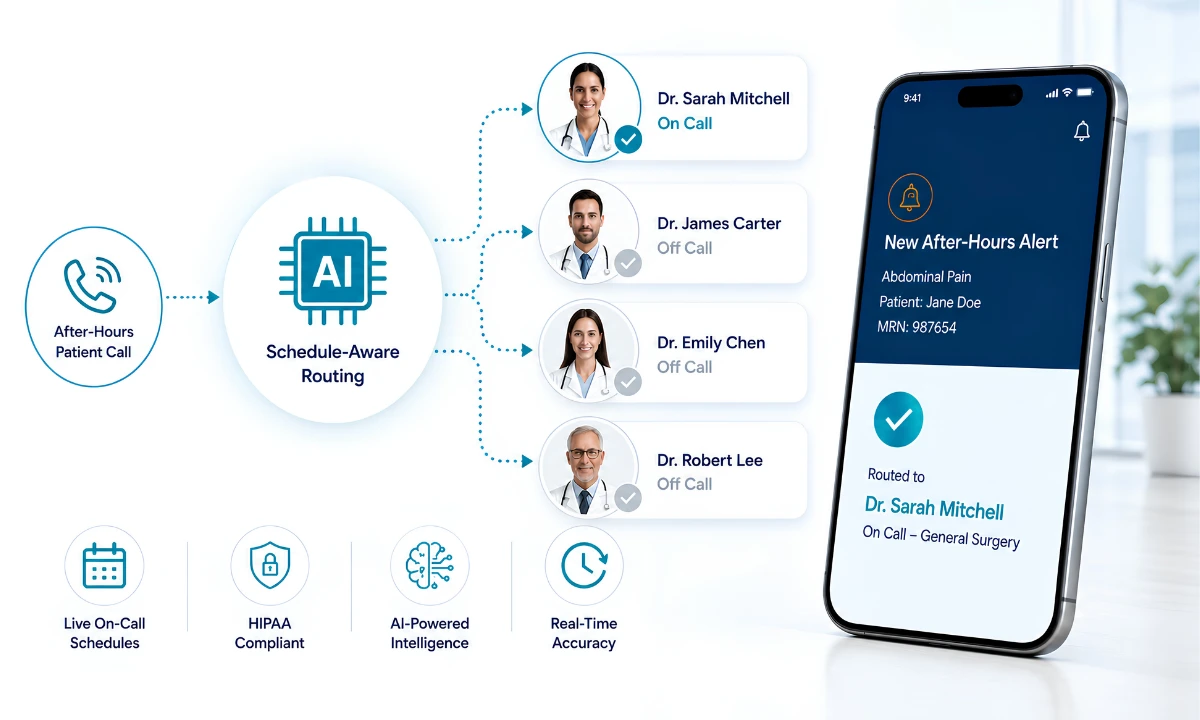
The HCO Practice HQ addresses intra-organizational communication: the routing, escalation, and distribution of clinical alerts and messages within a practice or hospital system. Smart routing logic reduces the alert overload that contributes directly to burnout. The HCO also reengages physicians through the use of personalized linear video and audio operations. It allows physicians to interact in an incredibly efficient and effective manner that forgoes the impersonal nature and delays of legacy systems. Physicians using the HCO Practice HQ have reported reclaiming 90 or more minutes per day previously consumed by unfiltered alert triage, clinical capacity returned to the practice without adding staff or changing workflows.
HCC: HealthCare Collaboration
The HCC Consult Core makes visible something that has been invisible in healthcare for decades: the informal consultation. Every physician knows the hallway consult. A specialist asked a quick question between cases. A curbside opinion offered in passing. These interactions carry genuine clinical value and have historically generated zero documentation and zero reimbursement. The HCC Consult Core changes that by supporting documented, billable interprofessional consultations using the active 2026 CPT code series: 99446 through 99449 for telephonic consultations, and 99451 and 99452 for written and internet-based consultations. MGMA data consistently shows that physician practices lose recoverable revenue annually to consultations that qualify for reimbursement but are never captured. HCC closes that gap without adding administrative burden to the physician’s workflow, which is central to the medical practice efficiency value we deliver to physician group practices.
The HCC Consult Core is also the pathway to physicians in other HCOs. Whether it is within your specialty or across specialties, the HCC connects physicians to other physicians on the network. This facilitates HealthCare collaboration on a whole new level. Consultations, case discussions, and patient transfers are all easily accomplished using the HCC.
HCX: HealthCare Xchange
The HCX Xchange provides a secure environment for compliant industry engagement. Physicians interact with the broader health ecosystem, including industry partners, pharmaceutical contacts, and health technology vendors. Those interactions carry compliance obligations under HIPAA and related federal regulations. HCX provides the structural compliance layer those interactions require, built into the platform architecture rather than managed as a separate process. You can learn more on the HCX platform page.
In the HCX, physicians can initiate and establish working relationships with trusted vendors without having to give up their own personal information to do so. Working directly with industry partners such as device manufacturers and pharmaceutical representatives eliminates much of the administrative sludge that prevents physicians from more efficiently and effectively bringing the most advanced treatment options to their patients.
Doc Lounge: Doctor’s Lounge
The Doc Lounge is a remembrance of where the platform began, and it remains its heart. It is a verified, physician-only peer community with specialty-specific forums, encrypted direct messaging, and even polling and voting capabilities. It is a space designed to rebuild the professional community that the disappearing doctors’ lounge once provided. This time, there are no administrators, no patient data, and no external interference.
It is a place where physicians can connect and engage. It is also a place where medical staff leaders can communicate and reunite with the medical staff in order to help them better represent the medical staff at the administrative level.
Taken together, these four modules form a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians. This is not a repurposed consumer application with a HIPAA addendum attached. It was designed from the first wireframe by a physician who knew exactly what was missing.
What This Journey Taught Me About Physician-Centered Design
Healthcare technology has a long history of being designed for the system and then handed to the physician. The EHR era produced tools optimized for billing capture and regulatory compliance, and physicians paid for that optimization with their time and their professional wellbeing. Research published in JAMA found that physicians spend nearly twice as much time on administrative tasks as on direct patient care, a ratio that has remained stubbornly resistant to incremental technology adjustments.
The Agency for Healthcare Research and Quality has documented that communication failures, not clinical errors alone, account for a substantial share of preventable patient harm events in U.S. healthcare settings. Communication infrastructure is not a secondary concern in medical practice. It is primary.
The lesson that I take from that evidence, and from the years of hypothesizing and testing a method to reengage physicians, is that addressing physician burnout requires returning clinical authority to the physician, starting with the tools they use to communicate. We must place physicians at the center of Healthcare communications.
The National Institutes of Health research has consistently linked structured interprofessional communication to measurable improvements in both patient safety outcomes and provider satisfaction. As we move from the benchtop to real clinical application, ClinicianCore now understands what unified clinical communication looks like at the practice level. This is where that conversation begins.
A secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians is not a peripheral feature in a modern medical practice. It is a structural requirement. When communication fails, care fails. When physicians are disconnected, decisions are slower and errors are more likely. When consultations go undocumented, clinical value disappears from both the patient record and the practice revenue cycle. When physicians are isolated burnout grows.
The soft launch of our HCO Practice HQ is scheduled for May 2026 with full platform availability in September 2026. The journey from that first rudimentary platform to a production-ready enterprise communication platform has taken years. However, with the addition of Neeraj, our CEO, Kris, our CTO, and our dedicated marketing and technical teams, we now understand that it will remain an ever-expanding project for years to come.
Still, despite our rapid growth, our mission has never changed. Our goal is to improve healthcare outcomes through a physician-designed, AI-powered, HIPAA-compliant communication and collaboration platform that enables secure, seamless, and efficient information exchange and interoperability for Doctors, Educators, Researchers, Clinicians, Diagnosticians and Administrators across the entire healthcare space.
We believe that the physicians, and all the professionals who work with them, deserve a communication and collaboration tool built by a healthcare team who understand what delivering care actually costs.
Frequently Asked Questions
What is ClinicianCore and who is it designed for?
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, serving physician group practices, outpatient clinics, and smaller community hospitals. It unifies four clinical communication modules within one application, addressing alert routing, interprofessional consultation documentation, compliant industry engagement, and peer community.
How does the Doc Lounge address physician isolation?
The Doc Lounge is a verified, physician-only peer community within ClinicianCore, providing specialty-specific forums, encrypted direct messaging, and community polling capabilities. It replaces the informal peer exchange that once occurred in physical doctors’ lounges, giving physicians a structured, secure space for clinical dialogue outside administrative and patient-facing channels.
What CPT codes does the HCC Consult Core support for interprofessional consultations?
The HCC Consult Core supports the active 2026 interprofessional consultation CPT code series: 99446 (telephonic, 5 to 10 minutes), 99447 (11 to 20 minutes), 99448 (21 to 30 minutes), 99449 (31 or more minutes), 99451 (consultant written consultation), and 99452 (requesting provider written consultation). These codes apply only to non-face-to-face remote consultations.
Why did physician burnout drive the creation of a communication platform specifically?
Communication dysfunction is one of the primary structural drivers of physician burnout, separate from workload volume. Fragmented tools, alert overload, and undocumented informal consultations each consume physician time and cognitive load without producing clinical or financial value. A unified communication platform addresses these structural causes rather than their symptoms.
How is ClinicianCore different from existing clinical communication tools?
ClinicianCore is a physician-designed clinical communication platform that unifies four distinct communication contexts in one HIPAA-compliant application, serving only physician-facing workflows with no patient-facing channels. Existing tools typically address one communication mode, are repurposed consumer applications, or were designed primarily for administrative or billing compliance rather than clinical workflow.