During my years in practice, first as an Air Force surgeon and later running an independent group, I operated under an unspoken rule: respond to everything immediately. Pages got answered within seconds. Phone calls got returned before rounds finished. The system was built around synchronous communication as the default, and no one questioned it, because urgency is core to what we do.
But urgency is not uniform. Not every message deserves an immediate response. When physicians default to real-time synchronous communication for all incoming clinical messages, regardless of actual time sensitivity, the result is a day structured entirely around interruption.
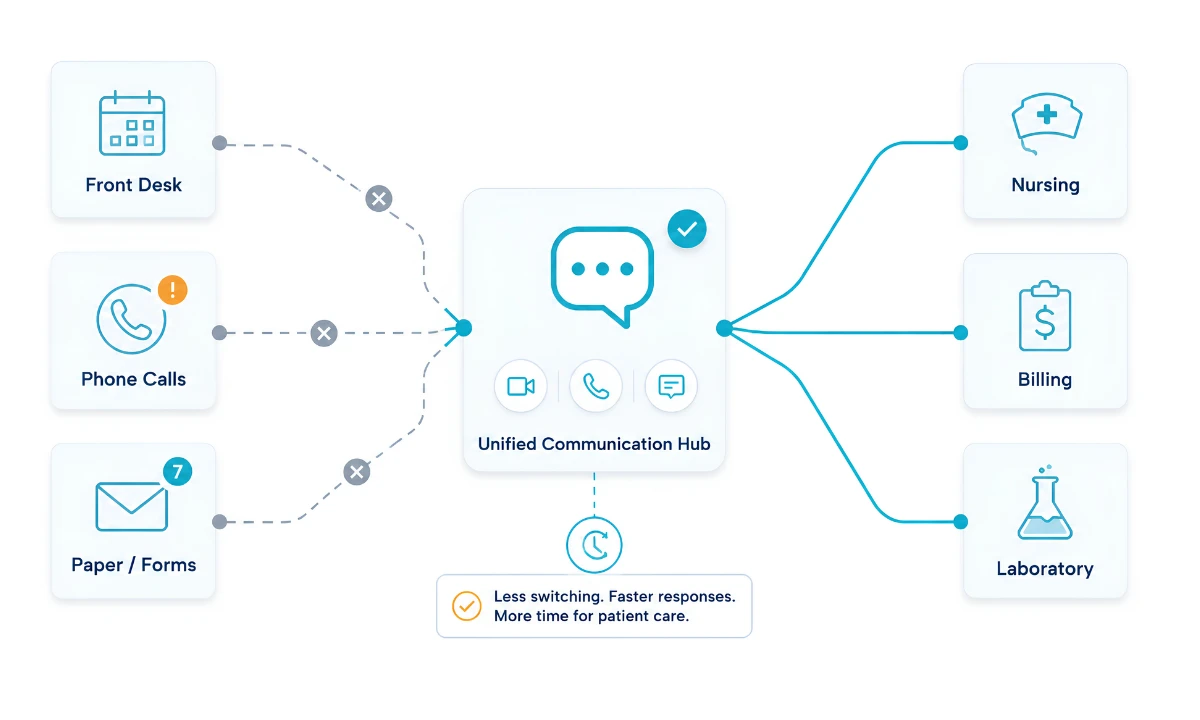
This is not a burnout article, though the connection is real. It is a workflow article about how I restructured the flow of communication in my practice by clearly distinguishing between what requires an immediate answer and what requires a thoughtful one at the right time. And how building that distinction into our system, using ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, changed what the rest of the day felt like.
Key Takeaways
- Synchronous and asynchronous communication serve different clinical functions. Treating all messages as equally urgent is the core workflow problem in independent physician practice.
- A 2021 study in BMJ Innovations (Jhala and Menon) found that shifting to an asynchronous clinical messaging platform reduced average task completion time by 20.1 minutes per interaction, a 58.8% improvement over traditional synchronous methods (p<0.01).
- AMA data shows physicians reported a 57.8-hour average workweek in 2024, with only 27.2 of those hours in direct patient care and 13 hours in indirect care tasks, including communication and coordination.
- Real-time communication is essential for clinical emergencies and time-critical decisions. The problem is using it as the default channel for all communication, regardless of urgency.
- Implementing a channel-routing framework requires documented criteria and team-wide alignment, not just a technology change.
“No single interruption is catastrophic. The pattern is.”

Real-Time Communication Is the Default, and That Is the Problem
In clinical environments, synchronous communication became the default because medicine often operates at the edge of urgency. You need a result now. You need a physician at the bedside now. The system trained us to respond in real time to everything because the cost of missing something urgent is high.
That conditioning is appropriate when the stakes are clinical. The problem is that it does not stop at the clinical threshold. A nurse confirming a routine medication time gets the same communication channel and the same response expectation as a nurse reporting a deteriorating patient. A colleague asking a scheduling question interrupts a focused documentation block with the same urgency signal as a critical lab value.
Research tracking inter-clinician communication across clinical settings found that 42% of all communication events were interruptions, with attending physicians experiencing these repeatedly throughout a shift, each lasting under a minute on average but occurring frequently enough to fragment sustained work (Edwards A, et al., Int J Med Inform, 2009).
According to the American Medical Association, physicians in 2024 reported an average workweek of 57.8 hours, with only 27.2 hours spent on direct patient care and 13 additional hours spent on indirect care tasks, including communication and documentation. When communication is interrupt-driven by default, those 13 hours compress and fragment in ways that make each individual task harder.
No single interruption is catastrophic. The pattern is.
When Real-Time Communication Is Non-Negotiable
Before building any communication framework, I found it necessary to define the categories where real-time is the only acceptable channel, not just understand them conceptually, but document them in a practical protocol.
Those categories are narrow and specific: acute patient deterioration, critical lab values requiring immediate action, any situation involving patient safety within the next 30 minutes, urgent coverage handoffs, and active care coordination where a delay could change a clinical outcome. These warrant a phone call, a direct message with immediate response expectation, or a face-to-face intervention. There is no substitute for synchronous communication in these moments.
The defining characteristic is time criticality, not clinical importance. Important information that does not require an answer within the next 30 to 60 minutes is not a real-time message, even if it will eventually affect patient care. Routine lab result review for stable patients, follow-up documentation requests, care coordination updates, and inter-office scheduling adjustments all meet that description.
Those categories cover the majority of what a physician receives in a day. Which means the majority of daily clinical communication does not require real-time response.
What Asynchronous Communication Does That a Phone Call Never Can
When a call interrupts a physician mid-task, the disruption cost is not just the time of the call. Returning to the prior task after any interruption requires additional cognitive effort beyond the interruption itself, which is why a one-minute page feels longer than it is.
A 2021 study published in BMJ Innovations followed healthcare professionals using a Time Motion Study methodology and found that shifting to an asynchronous clinical communication platform produced a 20.1 minute reduction in average task completion time per interaction, representing a 58.8% improvement over traditional synchronous methods (Jhala M, Menon R. BMJ Innov. 2021;7(1):68-74). The mechanism is not complex. When a physician responds to a non-urgent message on their own schedule, they bring full cognitive resources to that response. The communication is documented, searchable, and accountable.
Asynchronous communication also forces precision in a way that phone calls do not. Synchronous conversations allow ambiguity to persist. Written asynchronous messages require the sender to think through what they actually need before sending, which reduces redundant follow-up exchanges and creates a record that does not depend on memory.
These are the characteristics that informed the async care features in HCO Practice HQ. As a module within ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, HCO Practice HQ supports both real-time and asynchronous clinical workflows within a single HIPAA-compliant environment. Physicians are not choosing between speed and documentation. They are routing appropriately within one structured system. For the full framework of how this connects to unified communication design, see the unified clinical communication platform.
The Framework I Use to Route Every Communication in My Practice
The framework that restructured our communication comes down to a single routing question applied to every incoming or outgoing message:
Does this require a response that affects patient care in the next 30 minutes?
If yes, it routes through a synchronous channel. If no, it routes through a documented asynchronous channel. That question resolves most ambiguity without requiring physician involvement in the routing decision, because the rest of the team can apply it too. Nurses, medical assistants, and front desk staff can all evaluate an incoming communication against that single threshold.
Categories that consistently land in the asynchronous column include: routine medication clarifications, appointment rescheduling, lab result review for stable patients, referral coordination, prior authorization status, non-urgent prescription renewals, and inter-office care plan updates. These do not need to interrupt a physician who is in a patient encounter, in surgery, or in a focused documentation window.
Categories that consistently require real-time routing: critical lab values flagged for a patient under active care, urgent coverage requests, direct patient escalations, or any situation where the initiating party has identified immediate clinical risk.
The distinction is not always clean, particularly in high-volume practices. This is why the framework needs to be documented, tested in practice, and revisited as team composition and patient volume change. The goal is to reduce the number of situations that require judgment under interruption, not to eliminate judgment.
What Restructuring Looked Like in Practice and What Changed
The actual changes were less dramatic than the concept. We did not overhaul our EHR. We did not retrain the entire team in a week. We documented the routing decision criteria, ran two team meetings to walk through the logic with examples, and then observed where it broke.
It broke most often at the boundaries: situations where a team member was uncertain whether a message was time-critical and defaulted to synchronous communication out of caution. That is the correct default when uncertain. The framework does not eliminate judgment; it reduces the number of situations that require it. Over time, the team developed a shared vocabulary for communication urgency that made those boundary cases less frequent.
What changed in measurable terms: synchronous interruptions during patient encounters dropped. Documentation quality improved because physicians responded to messages with more complete information when they were not mid-task. Care coordination delays for non-urgent items decreased because asynchronous messages received responses in predictable windows rather than waiting for the right moment to make a call that kept getting postponed.
The less quantifiable change was the more significant one. Physicians in the practice reported feeling less reactive during patient care. The phrase that came up more than once: “I could finish a thought.” That is what removing interrupt-driven communication from non-urgent channels actually produces. Not more free time, but sustained focus when it matters most.
ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, was designed with exactly this kind of practice restructuring in mind. Its HCO Practice HQ module provides independent physician groups with the infrastructure to route urgent alerts in real time while ensuring non-urgent messages receive documented, audit-ready handling. If this framework reflects a problem you recognize in your own practice, the waitlist is open.
Frequently Asked Questions
What is the difference between asynchronous and real-time communication in a clinical setting?
Real-time (synchronous) clinical communication requires an immediate response from both parties: phone calls, direct conversations, and overhead alerts. Asynchronous communication allows the recipient to respond when available, such as secure messages or documented updates. ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, supports both within a single HIPAA-compliant system.
When should a physician use a phone call instead of a secure message during the workday?
Phone calls are appropriate when a response affects patient care within the next 30 minutes: critical lab values, acute deterioration, and urgent coverage needs. A 2021 BMJ Innovations study found shifting to asynchronous channels reduced task completion time by 20.1 minutes per interaction (p<0.01). ClinicianCore’s HCO Practice HQ applies this routing logic at the practice level.
How does excessive real-time communication contribute to physician burnout?
When synchronous communication is the default for all messages, attending physicians experience repeated interruptions throughout the day. Research tracking clinical communication events found that 42% were interruptions (Edwards et al., 2009), fragmenting the sustained focus periods physicians need for safe, effective care. ClinicianCore routes communication by urgency to reduce that pattern at the practice level.
Is asynchronous clinical communication HIPAA compliant?
Asynchronous clinical communication is HIPAA-compliant when conducted through an appropriately secured platform with access controls, encryption, and audit capabilities. Consumer messaging applications are not HIPAA compliant for clinical use, regardless of convenience. ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, supporting asynchronous messaging with full audit trails.
What steps can an independent physician group take to implement both asynchronous and real-time communication channels?
Independent physician groups can start by defining a routing threshold: which messages require a response within 30 minutes and which do not. Document these categories with team input, then select a HIPAA-compliant platform that supports both channel types. ClinicianCore’s HCO Practice HQ supports structured channel management for independent practice settings.