The United States is approaching a physician workforce crisis measured in decades. According to the Health Resources and Services Administration (HRSA), the country faces a projected shortage of 141,160 full-time equivalent (FTE) physicians by 2038, spanning 30 of 35 specialties evaluated. Independent group practices, already operating at the margins of administrative capacity, will absorb the greatest pressure from this deficit.
What this shortage demands is not simply more physicians. It demands a fundamentally more efficient use of the physicians who remain in practice. That efficiency begins with communication. When clinical communication is fragmented across consumer apps, paging systems, and siloed EHR portals, physician time disappears into coordination overhead rather than patient care.
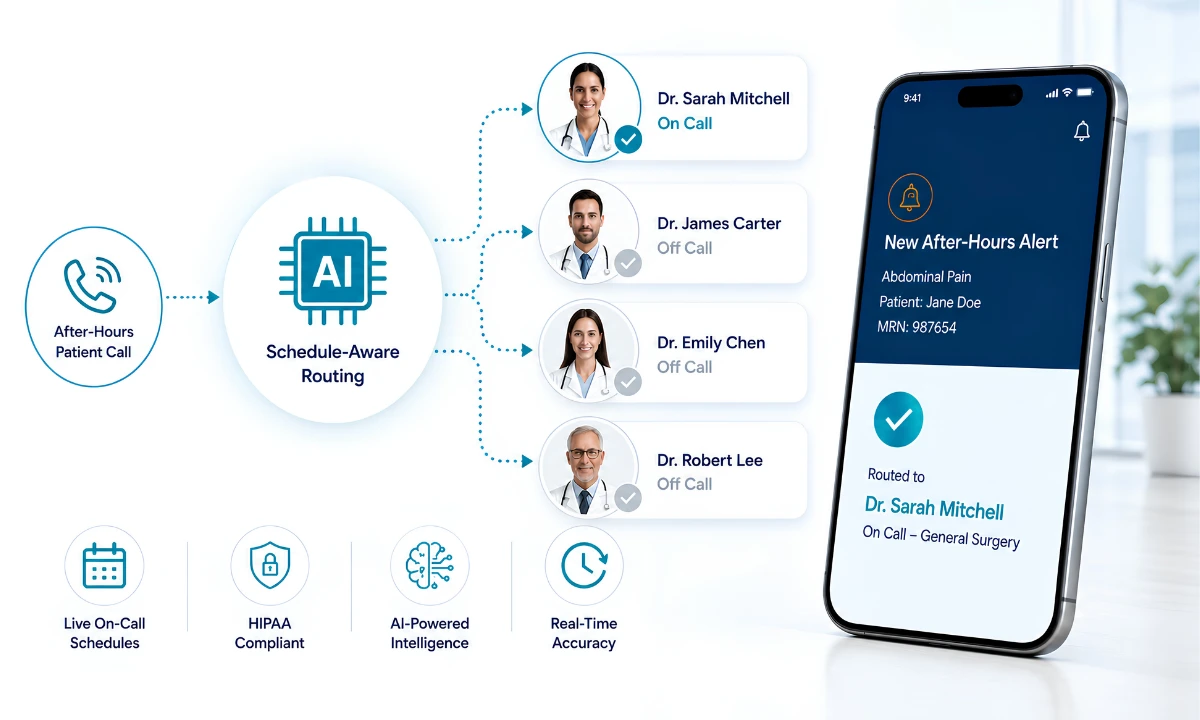
A unified clinical communication platform changes that calculus. By consolidating messaging, consultation documentation, and alert routing into a single HIPAA-compliant environment, independent practices can extend the effective capacity of their existing clinical staff, recover consultation revenue that currently goes unbilled, and reduce the administrative burden that accelerates early physician retirement.
This post examines the specific workforce pressures driving the 2038 shortage, the specialty-level data that defines where the gaps are most acute, and the communication infrastructure that gives independent practices a sustainable path forward.
Key Takeaways
- HRSA projects a shortage of 141,160 FTE physicians by 2038, affecting 30 of 35 specialties.
- Vascular surgery, ophthalmology, thoracic surgery, and family medicine face the steepest deficits.
- Non-metropolitan regions will experience disproportionately lower physician supply adequacy.
- Unified clinical communication platforms help independent practices maximize existing clinical capacity.
- CPT codes 99446-99449 and 99451-99452 make documented digital consultations billable revenue streams.
- Administrative fragmentation and professional isolation are primary accelerants of early physician retirement.
“Practices are already performing the clinical work that qualifies for reimbursement under CPT codes 99446 through 99452. The gap is not effort. It is documentation infrastructure. That gap is recoverable.”

The Scale of the 2038 Physician Shortage
The HRSA physician workforce projections, updated in December 2025, offer the most granular federal-level picture of where US healthcare is headed. The headline figure of 141,160 FTE physician deficit by 2038 obscures a more complex structural problem. This is not a uniform national shortage. It is a collection of specialty- and geography-specific deficits that are already compressing access to care in the communities that can least afford it.
HRSA’s simulation model evaluates supply adequacy as a percentage, where 100% represents a balanced state between physician supply and projected demand. Specialties falling below 100% face structural shortfalls that recruitment pipelines alone cannot close on relevant timelines. Medical school enrollment growth and residency expansion operate on 10 to 15-year lag cycles. The physicians who will be practicing in 2038 are, for the most part, already in training or already in practice.
This means independent group practices need solutions that work with the physician workforce that exists today. Operational efficiency, communication infrastructure, and documented consultation workflows are not luxuries for well-resourced health systems. They are survival tools for independent practices facing a decade-long workforce contraction.
At-Risk Specialties: Where the Deficit Is Most Severe
HRSA’s specialty-level projections reveal meaningful variation in which disciplines face the greatest pressure. Surgical subspecialties and primary care sit at opposite ends of the volume curve but share a common vulnerability: both operate in high-demand, high-documentation environments where communication inefficiency compounds clinical workload.
| Specialty | 2038 Supply Adequacy | Projected Shortage |
| Vascular Surgery | 66% | -34% |
| Ophthalmology | 72% | -28% |
| Thoracic Surgery | 73% | -27% |
| Plastic Surgery | 74% | -26% |
| Family Medicine | 76% | -24% |
| Hospital Medicine | 78% | -22% |
Vascular surgery’s 34% projected deficit is particularly consequential. Vascular surgical consultations frequently require real-time expert input across multiple care settings. When the specialist pool shrinks while demand grows, the ability to conduct rapid, documented interprofessional consultations — and bill appropriately for that time — becomes a core operational competency rather than an administrative convenience.
Family medicine faces a different dimension of the same problem. With a projected 24% deficit, primary care practices must serve larger patient panels with the same or fewer physicians. The administrative overhead of undocumented phone consultations, informal curbside advice, and fragmented follow-up communications directly reduces the number of patient encounters a practice can sustain per day. A secure HIPAA-compliant unified clinical communication platform built exclusively for physicians does not manufacture more clinical hours. It recovers hours that currently get lost to communication friction. For specialties under supply pressure, that recovery is measurable and material. See how our medical practice efficiency platform quantifies this capacity recovery for independent group practices.
Geographic Imbalance and Cross-Institutional Collaboration
The 2038 shortage is not evenly distributed across the country’s geography. HRSA projections show that non-metropolitan regions will experience substantially lower supply adequacy than urban centers — a projected 42% adequacy in nonmetro areas (a 58% shortage) compared to 95% adequacy in metro areas. Rural counties in states that already face primary care physician shortages will see those deficits widen as urban practices compete more aggressively for the same shrinking pipeline of graduates.
This creates a structural need for cross-institutional clinical collaboration that goes beyond what informal referral networks can support. A rural family practice managing a complex cardiology case cannot simply transfer every patient to an urban specialist. Patient transfers carry cost, risk, and care fragmentation. What they can do — if they have the right communication infrastructure — is conduct a real-time documented consultation with the appropriate specialist, regardless of physical location.
This is the core use case for the HCC Consult Core module inside ClinicianCore. HCC creates encrypted, HIPAA-compliant pathways that connect independent group practices across different networks. Critically, it captures clinical reasoning and decision trails natively, turning cross-institutional consultations into compliant, billable revenue streams under CPT codes 99446-99449 and 99451-99452.
The geographic imbalance in physician supply is not a problem that redistribution alone will solve. It requires a technology layer that makes geography less determinative of care quality. When a rural generalist can consult with a vascular surgeon two states away, document that consultation in a compliant platform, and bill appropriately for the encounter, the effective geographic reach of the specialist pool expands without requiring anyone to relocate.
How Unified Communication Extends Physician Capacity
The operational logic of unified clinical communication during a physician shortage is straightforward. Every minute a physician spends managing communication logistics — switching apps, waiting for pages to resolve, repeating clinical context across disconnected platforms — is a minute not spent in direct patient care. At scale, across a 12-physician group practice, this friction accumulates into measurable capacity loss.
Research from the American Medical Association and the University of Wisconsin, published in the Annals of Family Medicine, found that during a typical 11.4-hour primary care workday, physicians spent nearly six hours on EHR data entry and administrative tasks — representing approximately 52% of their clinical day. That figure encompasses documentation, order entry, billing-related tasks, and system navigation, and predates the further expansion of prior authorization requirements. For independent practices, coordination overhead is proportionally higher because they lack the dedicated administrative staff that large health systems deploy to absorb this burden.
The HCO Practice HQ module inside ClinicianCore addresses this directly. By consolidating video, voice, and text communication within the practice and applying intelligent alert routing, HCO helps existing personnel manage larger daily workflows without extending hours. Physicians receive prioritized, relevant communications rather than an undifferentiated stream of alerts that requires triage time at the individual level.
This operational efficiency compounds when combined with a cross-institutional consultation infrastructure. A practice that has eliminated internal communication friction and established documented pathways for specialist consultations operates with substantially greater effective capacity than its headcount alone suggests. That is the competitive and clinical advantage that a unified communication platform delivers during a period of constrained physician supply.
Recovering Consultation Revenue Through Documented Digital Consults
One of the least discussed consequences of physician workforce fragmentation is the systematic loss of consultation revenue that practices are already entitled to bill. Interprofessional consultations — the clinical discussions that happen between treating physicians and specialists about specific patient cases — have been billable under CMS since the introduction of the interprofessional consultation CPT code series.
The active billable codes for non-face-to-face remote consultations are:
- CPT 99446 — telephonic consultation, 5 to 10 minutes (requesting physician bills)
- CPT 99447 — telephonic consultation, 11 to 20 minutes (requesting physician bills)
- CPT 99448 — telephonic consultation, 21 to 30 minutes (requesting physician bills)
- CPT 99449 — telephonic consultation, 31 or more minutes (requesting physician bills)
- CPT 99451 — consulting specialist’s written or internet-based opinion
- CPT 99452 — requesting provider’s preparation and documentation time
Both the requesting and consulting physician can bill the same interprofessional consultation event. A patient visit is not required. What is required is a documented consultation with a written report — the precise workflow that a HIPAA-compliant collaboration platform is designed to capture.
For a 12-physician cardiology group conducting regular cross-specialty consultations that currently go undocumented, the revenue recovery opportunity is substantial. When consultation volume is tracked, documented in a compliant platform, and submitted against the appropriate CPT codes, practices recover revenue for clinical work they are already performing. This is not theoretical. The HealthCare Collaboration module captures consultation duration, clinical context, and written reports in a single workflow, generating the documentation required for CPT billing without adding administrative steps for the physician. See the full overview of the unified clinical communication platform to understand how HCC integrates into ClinicianCore’s broader communication architecture.
Reducing Burnout Through Structured Peer Networks
The HRSA shortage projection does not exist in isolation from physician retention trends. Administrative fatigue, professional isolation, and the absence of peer support channels are documented accelerants of early retirement among practicing physicians. The American Medical Association’s 2023 national physician comparison data found that 48.2% of physicians reported at least one symptom of burnout — down from 53% in 2022 but still representing nearly half the active physician workforce — with administrative burden consistently cited as the leading driver.
A shortage that is partly attributable to early retirement requires retention strategies alongside capacity solutions. Communication platforms that reduce administrative overhead address one dimension of this problem. But the professional isolation that characterizes independent practice — particularly in non-metropolitan settings — requires a different kind of infrastructure: a structured peer network where physicians can discuss clinical cases, share perspectives on operational challenges, and access collegial support without leaving their practice environment.
The Doc Lounge (Doctor’s Opinion Count) module inside ClinicianCore provides this environment. It is a physician-only peer community with specialty-specific forums designed for clinical discussion away from administrative oversight. Physicians can review complex cases, share perspectives on emerging clinical data, and engage with peers across specialties in a verified, secure environment. The Doc Lounge platform page details the forum structure and verification requirements for the physician-only community.
Professional isolation is a workforce retention problem. Structured peer networks are a retention solution. For independent practices that cannot replicate the collegial environment of academic medical centers or large hospital systems, a platform-embedded physician community closes a meaningful gap in the professional experience of independent practice. The broader context for these retention strategies is covered in ClinicianCore’s physician burnout reduction platform, which examines how communication infrastructure, alert management, and peer support work together to reduce the administrative pressures that drive early retirement.
A Communication Framework Built for the Physician Shortage Era
The HRSA projection of 141,160 FTE physician deficit by 2038 defines the scale of the challenge. Across the 30 specialties facing supply shortfalls, the combined projected deficit reaches 158,990 FTE physicians when surgical subspecialties are aggregated. No recruitment initiative, medical school expansion, or residency program modification will close a gap of that magnitude within the remaining timeline.
What independent practices can control is how efficiently their existing physicians operate. Communication infrastructure is not peripheral to that efficiency. It is central to it. When physicians spend less time on coordination overhead, more clinical time becomes available. When cross-institutional consultations are documented and billed, practices recover revenue that currently subsidizes unreimbursed clinical work. When professional isolation is reduced through structured peer networks, retention improves, and the workforce projection improves alongside it.
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians. Its four modules — HCO for intelligent alert routing, HCC for billable interprofessional consultation documentation, HCX for multi-channel secure communication, and Doc Lounge for physician peer community — address the specific operational pressures that a shrinking physician workforce creates for independent group practices.
The practices that will navigate the 2038 workforce constraints most effectively are those that build their communication infrastructure now, before the shortage deepens. The investment in unified clinical communication is not a hedge against uncertainty. It is a response to a projection that federal workforce modeling has already confirmed. Explore the complete framework on the unified clinical communication platform page or review the HIPAA-compliant collaboration platform to understand how compliance infrastructure supports sustainable cross-institutional practice.
Frequently Asked Questions
How does unified clinical communication reduce physician burnout during a shortage?
Unified clinical communication reduces physician burnout by consolidating fragmented messaging, alerts, and consultation workflows into a single HIPAA-compliant platform. Physicians spend less time switching between apps, reducing cognitive load. AMA data shows administrative tasks consume roughly 52% of physician workdays. ClinicianCore addresses this directly through integrated routing and documentation tools.
What physician specialties face the most severe workforce shortages by 2038?
HRSA projects vascular surgery (-34%), ophthalmology (-28%), thoracic surgery (-27%), and family medicine (-24%) as the hardest-hit specialties by 2038. These surgical and primary care disciplines face the steepest supply deficits, requiring practices to maximize existing physician capacity through efficient communication and cross-institutional collaboration tools.
Can interprofessional consultation platforms help independent practices manage physician shortages?
Yes. Interprofessional consultation platforms allow independent practices to access remote specialist expertise without adding headcount. HRSA data shows that non-metropolitan areas will experience below-average supply adequacy by 2038. HIPAA-compliant platforms like ClinicianCore enable billable cross-institutional consults under CPT codes 99446-99449 and 99451-99452, creating documented, reimbursable pathways for distributed care.
How does HIPAA-compliant messaging differ from consumer apps for clinical communication?
HIPAA-compliant messaging platforms encrypt PHI in transit and at rest, maintain audit trails, and enforce access controls required under the HIPAA Security Rule. Consumer apps like iMessage and WhatsApp lack these protections. IBM’s 2023 Cost of a Data Breach Report found the average healthcare data breach cost $10.93 million, making HIPAA-compliant infrastructure a financial imperative.
What CPT codes apply to remote interprofessional consultations between physicians?
CPT codes 99446 through 99449 cover telephonic interprofessional consultations from 5 to 31+ minutes. CPT 99451 reimburses the consulting specialist’s written or internet-based opinion. CPT 99452 reimburses the requesting provider’s preparation time. Both the requesting and consulting physician can bill the same consultation event, making documented digital consults a recoverable revenue stream.
References
- Health Resources and Services Administration. (December 2025). Physician Workforce: Projections, 2023-2038. National Center for Health Workforce Analysis. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/data-research/physicians-projections-factsheet.pdf
- Sinsky C, Colligan L, Li L, et al. (2016). Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 Specialties. Annals of Internal Medicine, 165(11), 753-760. https://doi.org/10.7326/M16-0961
- American Medical Association. (2024). Physician Burnout Rate Drops Below 50% for First Time in 4 Years. AMA. https://www.ama-assn.org/practice-management/physician-health/physician-burnout-rate-drops-below-50-first-time-4-years
- IBM Security. (2023). Cost of a Data Breach Report 2023. IBM. https://www.ibm.com/reports/data-breach
- Dai M, Ingham RC, Peterson LE. (2019). Scope of practice and patient panel size of family physicians who work with nurse practitioners or physician assistants. Family Medicine, 51(4), 311-318. https://doi.org/10.22454/fammed.2019.438954 [Note: Pre-2023 — replace with 2023+ equivalent when available]
- Peikes DN, Reid RJ, Day TJ, et al. (2014). Staffing patterns of primary care practices in the Comprehensive Primary Care Initiative. Annals of Family Medicine, 12(2), 142-149. https://doi.org/10.1370/afm.1626 [Note: Pre-2023 — replace with 2023+ equivalent when available]
- Pineda A. (2026). Addressing national health care needs: recent US MD graduates and their intention to practice in underserved areas. Academic Medicine, 101(2), 214.
- Centers for Medicare and Medicaid Services. (2026). Physician Fee Schedule 2026 Final Rule. CMS. https://www.cms.gov/medicare/physician-fee-schedule/pfs-federal-regulation-notices
- National Academies of Sciences, Engineering, and Medicine. (2023). Implementing High-Quality Primary Care: Rebuilding the Foundation of Health. The National Academies Press. https://doi.org/10.17226/25983