What Is Unified Clinical Communication Architecture?
A centralized healthcare communication framework that integrates secure messaging, EHR interoperability, intelligent alert routing, and compliance governance into a unified operational layer.
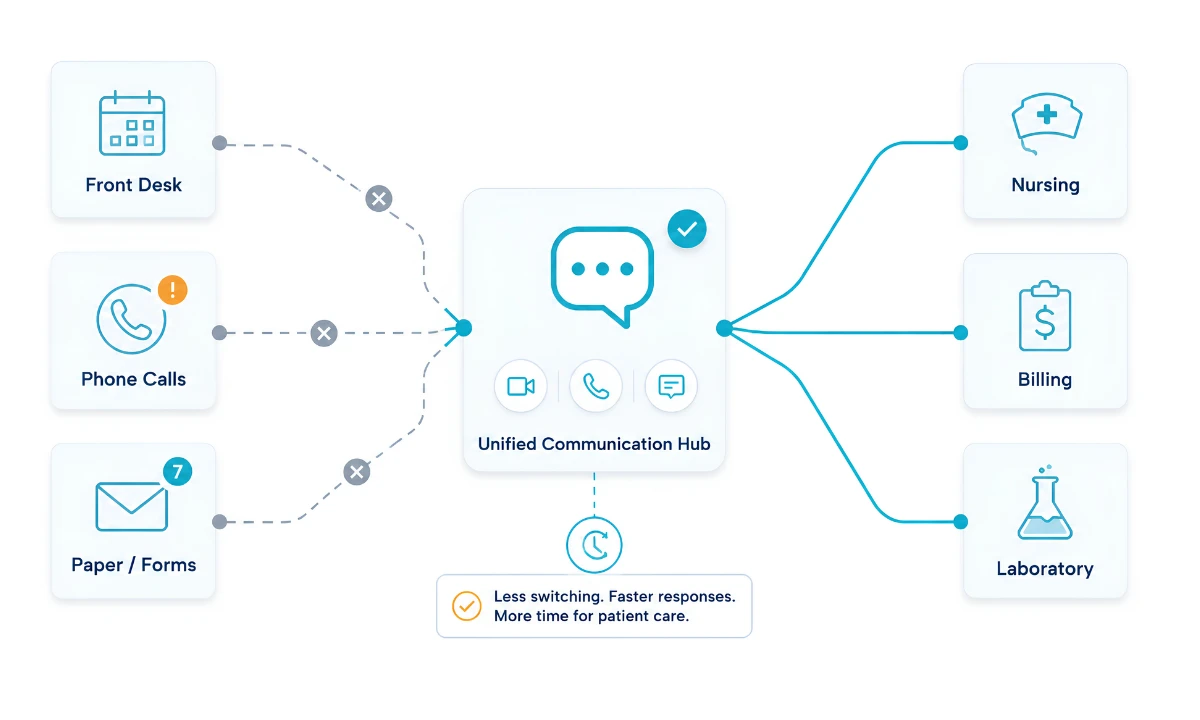
In most healthcare settings, critical patient information still travels through a patchwork of pagers, secure messaging apps, EHR alerts, and phone calls. While each tool serves a purpose, the lack of structural integration creates hidden delays, cognitive overload, and compliance risk.
A unified clinical communication architecture addresses this fragmentation by redesigning healthcare communication as a centralized operational layer, one that integrates secure messaging, EHR interoperability, intelligent alert routing, and governance controls into a cohesive operational framework.
Example Scenario:
If a critical potassium value is reported at 2:00 AM, a fragmented system may require manual paging, phone callbacks, and EHR login verification, introducing a 20–40 minute delay. In a unified architecture, that value is automatically contextualized, routed to the on-call physician, and documented in the audit log within seconds.
Key Takeaways
| Core Concept | What It Means in Practice | Strategic Impact |
|---|---|---|
| Infrastructure, Not Apps | Communication must function as an integrated system layer rather than standalone tools | Reduces fragmentation and systemic delays |
| Interoperability as Foundation | HL7 and FHIR enable structured, bi-directional data exchange with the EHR | Eliminates manual re-entry and workflow friction |
| Intelligent Alert Routing | Role-based and context-aware escalation replaces static paging | Reduces alarm fatigue and cognitive overload |
| Governance & Audit Controls | Centralized logging, lifecycle management, and compliance enforcement | Strengthens HIPAA compliance and enterprise risk mitigation |
| Executive-Level Impact | Communication architecture influences LOS, bed turnover, and operational throughput | Supports value-based care and financial performance |
Why Healthcare Communication Must Be Designed as Infrastructure
Historically, healthcare organizations have treated clinical communication as a series of standalone applications. A hospital might utilize legacy paging systems for emergency alerts, secure text messaging applications for physician-to-physician consults, and distinct, siloed software for nurse call systems.
Clinical communication failures have been shown to directly impact patient safety and operational efficiency across health systems. The Agency for Healthcare Research and Quality (AHRQ) has consistently identified communication breakdowns as a contributing factor in preventable adverse events, reinforcing the need for systemic rather than incremental solutions.
Research published by The Joint Commission has identified communication breakdown as a leading root cause of sentinel events in U.S. hospitals, contributing to a significant percentage of preventable adverse outcomes. These findings reinforce that communication inefficiency is not merely an operational inconvenience but a systemic patient safety risk that requires architectural intervention rather than incremental tool adoption.
To achieve systemic efficiency, healthcare communication must be fundamentally redesigned using infrastructure-level design thinking. Just as a hospital facility relies on integrated HVAC, plumbing, and electrical grids, clinical operations require a comprehensive data and communication grid. Treating communication as infrastructure means establishing a unified clinical communication architecture that centralizes the routing, processing, and delivery of all clinical data across hospital communication systems.
When communication is architected as an infrastructure layer, it standardizes the protocols by which information travels. It eliminates “shadow IT”—the unauthorized use of consumer-grade messaging apps by clinicians desperate for faster communication. Infrastructure design thinking demands high availability, redundancy, and interoperability. It requires systems that can ingest a critical lab value from an LIS (Laboratory Information System), cross-reference it with the on-call schedule, format it securely, and deliver it to the precise attending physician’s mobile device, all within milliseconds. This level of orchestration is mathematically and technically impossible without a centralized architectural foundation designed specifically for the complexities of modern clinical environments.
The Four Layers of Unified Clinical Communication Architecture
A robust communication architecture framework is constructed through four distinct but deeply interconnected technological layers.
1. The Secure Layer
At the foundational level is the secure layer. Healthcare data is among the most sensitive and highly targeted information globally. Therefore, the architecture must operate on a Zero Trust Network Access (ZTNA) model, assuming no device or user is inherently secure until authenticated.
This layer encompasses end-to-end encryption protocols (such as AES-256 for data at rest and TLS 1.3 for data in transit). It also dictates mobile device management (MDM) compatibility, ensuring that whether a hospital uses shared ward devices or a Bring Your Own Device (BYOD) policy, the communication architecture can isolate clinical data from personal data. Identity and Access Management (IAM) is structurally embedded here, relying on biometric authentication, Single Sign-On (SSO), and rapid re-authentication protocols that accommodate the fast-paced physical movement of clinicians throughout a facility.
To effectively protect patient data across diverse endpoints, organizations must adopt a Zero Trust healthcare architecture. In modern clinical environments where providers transition constantly between shared workstations, personal devices, and remote networks, no device or user can be inherently trusted. Continuous authentication, contextual authorization, and strict identity validation prevent lateral movement within hospital communication systems, ensuring that even compromised credentials cannot propagate risk across the enterprise.
2. The Workflow Integration Layer
Security without usability severely degrades clinical operations. The workflow integration layer is the connective tissue between the unified clinical communication architecture and the broader hospital ecosystem.
This layer relies heavily on interoperability standards such as HL7 (Health Level Seven) and FHIR (Fast Healthcare Interoperability Resources). Through bidirectional API gateways, the communication architecture interfaces directly with the EHR, physiological monitors, nurse call systems, and bed management software. For example, rather than a nurse manually transcribing a patient’s deteriorating vitals into a message, the workflow integration layer automatically extracts the relevant vitals, links them to the patient’s EHR profile, and delivers a highly contextualized alert to the appropriate rapid response team.
Within a modern healthcare IT infrastructure, this interoperability eliminates the need for manual data transcription between systems. HL7 FHIR communication acts as a universal translator, allowing structured, discrete patient data elements to flow securely between EHR platforms, laboratory systems, and monitoring devices without creating additional administrative burden.
3. The Collaboration Intelligence Layer
The third tier shifts the architecture from passive routing to active assistance. The collaboration intelligence layer focuses on contextualizing the delivery of information to optimize human response.
This is where healthcare AI integration in communication becomes highly relevant. Advanced algorithms analyze the urgency of incoming data against the real-time availability and workload of clinical staff. This layer powers dynamic role-based routing; a message sent to “Cardiologist On-Call” is automatically directed to the correct physician based on live scheduling data, rather than requiring the sender to look up a specific name. Furthermore, natural language processing (NLP) can parse text to identify critical keywords, automatically escalating the priority of the notification and overriding “Do Not Disturb” settings for life-threatening scenarios, such as a Code Blue or an acute sepsis alert.
This layer also directly supports alarm fatigue solutions through intelligent prioritization and context-aware routing. Rather than broadcasting every alert indiscriminately, the system evaluates clinical severity, role responsibility, and provider workload before escalation. Routine notifications can be batched for later review, while life-threatening alerts override suppression thresholds. This architectural filtering reduces cognitive noise and preserves clinician attention for events requiring immediate intervention.
4. The Governance Layer
The final layer sits atop the system to monitor, audit, and optimize the entire framework. The governance layer provides the administrative control required for enterprise deployment.
It manages the data lifecycle, dictating how long messages are retained to comply with legal holds and when they are automatically purged to minimize liability. It provides robust analytics dashboards that measure system performance, message delivery latency, and user adoption rates. Most importantly, the governance layer generates immutable audit logs that record precisely who accessed what data, when it was accessed, and where it was routed, creating a transparent ecosystem that protects both the patient and the institution.
The Four-Layer Unified Clinical Communication Architecture Framework

- Security Foundation Layer – Encryption, identity validation, and Zero Trust enforcement
- Interoperability Engine – HL7 FHIR communication and EHR integration
- Collaboration Intelligence Layer – Dynamic routing, prioritization, and workload awareness
- Governance & Audit Layer – Compliance monitoring, analytics, and lifecycle management
Outcome: Reduced clinical latency, optimized workflow execution, improved compliance integrity, and lower cognitive load across interdisciplinary teams.
Fragmented vs Unified Communication Systems
To fully understand the necessity of a unified clinical communication architecture, it is essential to compare the structural differences between traditional fragmented environments and fully unified systems.
| Architectural Dimension | Fragmented Communication Systems | Unified Clinical Communication Architecture |
| System Interoperability | Siloed; requires manual data entry and copying between disparate applications. | Deeply integrated via HL7/FHIR; bi-directional syncing with the EHR. |
| Alert Routing | Static and manual; relies on printed schedules and centralized switchboards. | Dynamic and intelligent; role-based routing connected to live on-call directories. |
| Clinical Context | Low; messages often lack patient IDs, requiring clarification and delays. | High; messages natively include embedded patient data, lab results, and history. |
| Security & Compliance | Inconsistent; high risk of shadow IT and unsecured SMS usage. | Uniformly enforced; centrally managed encryption, SSO, and secure data sandboxing. |
| Cognitive Load | High; clinicians suffer from alarm fatigue and excessive context switching. | Optimized; intelligent alert filtering prioritizes critical data and minimizes noise. |
| Analytics & Auditing | Disjointed; impossible to track a full communication lifecycle across platforms. | Centralized; comprehensive auditing, eDiscovery, and performance metrics. |
The comparative data reveals that fragmented systems introduce latency into critical care pathways. When a clinician must log out of a secure messaging app, log into the EHR to verify a patient’s weight, and then call a pharmacy, the architecture itself becomes a barrier to patient care. A unified model collapses these steps into a single, seamless workflow.
Clinical Workflow Optimization Through Architectural Design
True clinical workflow optimization is achieved through structural engineering rather than behavioral mandates. When communication systems are fragmented, inefficiencies are embedded into daily clinical processes. A unified architecture streamlines data retrieval, contextual alert delivery, and documentation workflows at the infrastructure level, allowing clinicians to operate within a coherent operational framework instead of compensating for technological gaps.
The design of clinical systems has a profound, measurable impact on the psychological and physiological well-being of medical professionals. The modern hospital environment bombards clinicians with an overwhelming volume of auditory and digital alerts. This phenomenon, known as alarm fatigue, occurs when the sheer volume of low-priority notifications desensitizes staff, leading to delayed responses to genuinely critical events.
From an architectural standpoint, an unoptimized system constantly interrupts a physician’s flow state. Every time a clinician has to context-switch—moving from diagnosing a patient to answering a non-urgent text, to logging back into an EHR—cognitive friction increases. Chief Medical Officer Dr. Kevin D. Halow, MD, MBA, has highlighted that clinical fatigue is frequently rooted in poorly designed workflows rather than simply an excess of work. When technology requires clinicians to perform the heavy lifting of data gathering and synthesis, it depletes the cognitive reserves required for actual patient care.
A well-designed communication framework acts as a structural intervention that reduces systemic cognitive strain within clinical workflows.
By delivering the right information, to the right person, at the exact right time—and suppressing the rest—the architecture fundamentally reduces the cognitive processing required by the physician. They no longer have to synthesize fragmented data; the system presents a holistic clinical picture, allowing the physician to focus entirely on medical decision-making.
This systemic strain has been identified as a major contributor to organizational burnout patterns across healthcare systems.
HIPAA Within Communication Architecture
In healthcare, regulatory compliance is non-negotiable, and the Health Insurance Portability and Accountability Act (HIPAA) heavily dictates technological infrastructure. However, an effective architecture distinguishes between the technical mechanisms of security and the administrative frameworks of governance.
To establish a true HIPAA compliant collaboration framework, an architecture must address the Technical, Physical, and Administrative Safeguards mandated by the law.
Technically, the system must prevent unauthorized access to Protected Health Information (PHI). This is achieved through the secure layer’s encryption protocols and authentication requirements. If a clinician’s mobile device is lost or stolen, the architecture allows administrators to remotely wipe the clinical application without affecting the user’s personal data, ensuring no PHI is compromised.
Administratively, HIPAA requires strict auditing and access controls. The governance layer of the unified clinical communication architecture automatically logs every interaction with PHI. It tracks when a message was sent, delivered, read, and archived. Furthermore, the architecture facilitates the enforcement of Business Associate Agreements (BAAs) with cloud service providers and vendors by providing the necessary transparency and reporting capabilities.
Crucially, an optimized architecture prevents the accidental violation of HIPAA by making the secure workflow the path of least resistance. When secure, unified communication is faster and easier to use than standard SMS, clinicians naturally adopt the compliant system, drastically reducing the organization’s risk profile.
Executive Implications of Communication Architecture
For healthcare executives, investing in unified clinical communication infrastructure is a macro-level strategic decision that impacts financial stability, operational efficiency, and clinical outcomes.
The transition to a unified communication infrastructure represents a structural clinical optimization initiative rather than a conventional IT upgrade.
As noted by CEO Neeraj Jain, structural investments in communication technologies are directly linked to enterprise-wide operational performance. When communication architectures are fragmented, the inefficiencies manifest financially. Delayed communication leads to increased patient length of stay (LOS), slower bed turnover rates, and delayed discharges. A nurse waiting 45 minutes for a physician to respond to a fragmented page regarding a discharge order is 45 minutes a bed remains occupied, directly impacting hospital revenue.
For example, reducing average critical alert response time from 18 minutes to under 5 minutes can materially impact patient throughput and clinical outcomes in high-acuity environments.
Implementing an integrated communication framework facilitates highly accurate medical practice efficiency modeling. Executives can utilize the data generated by the governance layer to identify communication bottlenecks. They can track the exact average response time for critical lab alerts across different departments and implement targeted process improvements.
Furthermore, unified architecture significantly mitigates institutional risk. By enforcing centralized security, organizations protect themselves from the financial and reputational devastation of data breaches and HIPAA fines.
Ultimately, building a structurally unified communication framework is a requirement for health systems seeking to transition toward value-based care, as it provides the necessary agility to coordinate complex, interdisciplinary patient management effectively.
Communication Architecture as a Strategic Asset in Value-Based Care
In value-based care environments, communication architecture directly influences clinical throughput, risk mitigation, and financial performance. Fragmented hospital communication systems introduce invisible latency into discharge coordination, specialist consultations, and interdisciplinary case reviews.
A structurally unified architecture reduces patient length of stay (LOS) by accelerating clinical decision pathways. When discharge approvals, laboratory confirmations, and specialty consultations are routed intelligently, bed turnover improves without expanding physical capacity.
From a financial modeling perspective, centralized governance analytics allow executives to quantify communication latency and identify operational bottlenecks. By measuring response time variance across departments, healthcare leaders can implement targeted structural optimizations.
Beyond operational efficiency, unified communication architecture mitigates institutional compliance risk. Centralized auditing, encryption enforcement, and role-based access controls significantly reduce HIPAA exposure and reputational vulnerability.
In this context, communication infrastructure becomes a strategic asset supporting coordinated, interdisciplinary care delivery within complex healthcare ecosystems.
Frequently Asked Questions
What is a unified clinical communication architecture?
It is an enterprise-wide technological infrastructure that consolidates healthcare messaging, clinical alerts, EHR data, and on-call scheduling into a single, integrated platform to streamline secure clinical collaboration.
How does communication architecture impact patient safety?
By eliminating manual data entry and disjointed phone calls, a unified architecture accelerates the delivery of critical clinical information (like sepsis alerts or critical lab results) directly to the right caregiver, significantly reducing the time to intervention and preventing medical errors.
What role does interoperability play in this architecture?
Interoperability standards, specifically HL7 and FHIR, are the foundation of the workflow integration layer. They allow the communication system to seamlessly “talk” to the EHR, laboratory systems, and medical devices, ensuring data flows bi-directionally without friction.
Can an optimized architecture really reduce physician burnout?
Yes. Fragmented systems cause alarm fatigue and force clinicians to constantly context-switch. A unified architecture uses intelligent routing to filter out noise, delivering only relevant, contextualized data, which significantly lowers the daily cognitive load on medical staff.
What is the difference between an app and clinical communication infrastructure?
An app is a standalone software tool meant for a specific task (like texting). Infrastructure is a foundational, system-wide framework that orchestrates all data flows, integrates with existing hardware and software, and centrally manages security, routing, and governance across the entire hospital ecosystem.
How does a unified architecture enforce HIPAA compliance?
It natively embeds technical safeguards like end-to-end encryption and automatic log-offs, while providing administrative safeguards such as comprehensive audit trails, remote device wiping capabilities, and strict, role-based access controls to protect all PHI.