In surgery, we say time is tissue. The principle holds equally for consultation medicine: every hour between a patient’s need for specialist input and the actual clinical exchange is an hour in which care decisions are made without complete information. Specialist consultation delays are not a peripheral inconvenience. They are documented patient safety events that increase diagnostic error rates, extend hospital length of stay, and contribute to preventable readmissions.
After more than two decades in clinical practice, including surgical service in the United States Air Force, I co-founded ClinicianCore because I recognized that communication infrastructure, not specialist availability, was the primary driver of consultation delay. The research increasingly confirms that observation. This post examines specialist consultation delays patient outcomes through the 2026 evidence, identifies the structural mechanism behind those delays, and outlines the solution that practitioners and practice administrators can act on. For an overview of the platform that addresses this gap, visit the unified clinical communication platform.
Key Takeaways
-
- Specialist consultation delays are primarily driven by communication friction in the initiation and routing of requests, not by specialist unavailability.
-
- Approximately 1 in 20 US adults experiences a diagnostic error in the outpatient setting annually, with delayed or absent specialist input identified as a key structural contributing factor (Singh et al., BMJ Quality and Safety, 2014).
-
- The Joint Commission identifies communication failures as the leading contributing root cause in sentinel events, including cases where delayed consultation contributed to adverse outcomes.
-
- Phone-based and fax-based consultation initiation creates a measurable lag between the treating physician’s request and the specialist’s informed response.
-
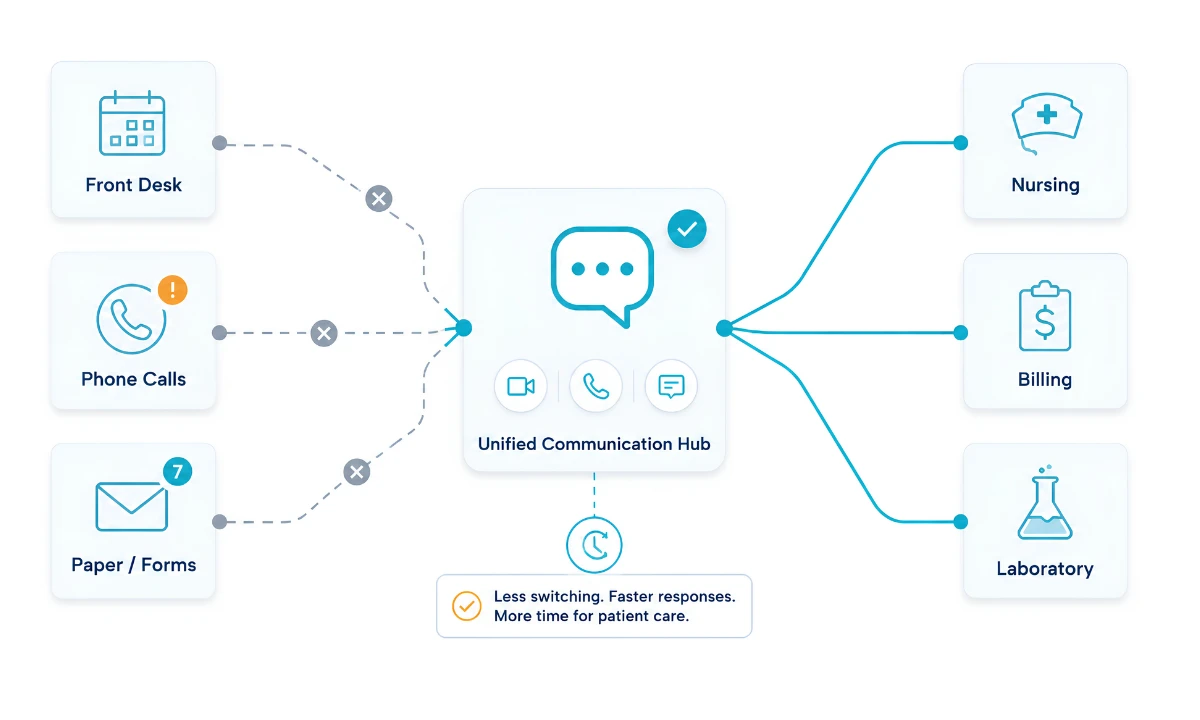
- ClinicianCore HCC replaces the phone-and-fax consultation loop with a structured, documented channel that captures requests, clinical context, and specialist responses in a single auditable thread.
“In surgery, a delayed consult is never just an administrative inconvenience. It is the time a patient spends without the right clinical input. Time, in medicine, is tissue, and we cannot afford to lose it to a broken phone loop.”

Specialist Consultation Delays Patient Outcomes: What the Evidence Shows
Specialist consultation is a core mechanism of inpatient and outpatient care. A treating physician identifies a clinical question outside their specialty domain and initiates a request for expert input. The specialist reviews the case, provides a clinical assessment, and the treating physician integrates that input into the care plan. In theory, this process is efficient. In practice, it is reliably delayed.
The 2015 National Academies of Sciences, Engineering, and Medicine (NASEM) report, Improving Diagnosis in Health Care, established that diagnostic error is among the most significant and under addressed patient safety challenges in the United States. The report documented that most Americans will experience at least one diagnostic error in their lifetime, and that failures in the consultation process, including delayed specialist access, incomplete information transfer at referral, and absence of structured documentation, are contributing factors (NASEM, 2015).
Singh and colleagues (2014), in a landmark study published in BMJ Quality and Safety, estimated that approximately 1 in 20 US adults experiences a diagnostic error in the outpatient setting each year. That figure represents millions of individuals annually. Clinical communication failures at the interface between the treating provider and the consulting specialist represent a structural vulnerability in the diagnostic process, one that is both measurable and addressable.
The Joint Commission has consistently identified communication failures as the leading contributing root cause in reported sentinel events. Cases in which delayed specialist input contributed to diagnostic error or treatment delay appear in this data with regularity. Bates and colleagues (2023), publishing in the New England Journal of Medicine, identified at least one adverse event in 23.6% of inpatient admissions, nearly one in four, and found that approximately one quarter of those events were preventable.
For a broader analysis of how structural communication failures affect care outcomes, see our overview of clinical communication failures in healthcare.
The True Cause of Delay: Communication Friction, Not Specialist Availability
The instinctive explanation for specialist consultation delays is supply-side: not enough specialists, too many patients, insufficient coverage. The data does not support this as the primary mechanism. Research on consultation turnaround times consistently identifies the initiation phase, the period between when the treating physician decides to consult and when the specialist receives a complete clinical handoff, as the primary source of delay.
Phone-based consultation initiation is the dominant model in most US physician practices and community hospitals. The treating physician places a call. The specialist is unavailable. A message is left through an answering service, a paging system, or a nurse intermediary. The specialist calls back. The treating physician is now with a patient. A second exchange is attempted. Clinical context is compressed into a verbal summary without documentation. The specialist asks follow-up questions that require another call. Total elapsed time before the specialist has enough information to render a meaningful clinical opinion: hours. In some cases, days.
Fax-based referral compounds the problem in outpatient consultation workflows. Referral documents are sent without confirmation of receipt. Specialists receive incomplete clinical summaries. Follow-up requires a phone call back to the referring practice. The consultation loop itself becomes a source of administrative overhead that delays care for the patient who initiated it and for every patient queued behind them.
This is a communication design failure. The specialist was available. The clinical need was identified. The gap was in the mechanism used to connect them.
ClinicianCore HCC, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, replaces the phone-and-fax initiation loop with a structured, documented consultation request that carries the patient’s clinical context from the treating physician to the specialist in a single, real-time or asynchronous thread. No phone tag. No lost fax. No verbal summary compressed under time pressure. The request is sent. The specialist receives it with clinical context intact. The response is documented. Both parties have a shared, auditable record. Visit the HealthCare Collaboration platform for full module details.
How Delays Translate to Clinical Harm
Diagnostic Error
The connection between delayed specialist consultation and diagnostic error is direct. The connection between delayed specialist consultation and diagnostic error is direct. When specialist input arrives after initial treatment decisions are already in motion, the treating physician may have committed to a diagnostic hypothesis without the corrective lens of expert review. The specialist’s subsequent assessment may identify a discrepancy, but only after orders have been written, treatments begun, or discharges planned. In time-sensitive conditions, including sepsis, pulmonary embolism, and acute cardiac events, that sequence carries direct consequences.
The NASEM (2015) report clearly frames this: diagnostic errors frequently occur at the interface between specialties when care transitions lack structured communication. Specialist consultation delays extend the window in which a patient is managed on the basis of incomplete diagnostic information. The Agency for Healthcare Research and Quality (AHRQ) Patient Safety Network catalogs diagnostic delay as a recurring theme in adverse event reporting, with consultation initiation failures appearing consistently across event types.
Extended Length of Stay
Length of stay in the inpatient setting is directly affected by consultation turnaround time. A patient admitted for a surgical complaint who requires a nephrology consultation cannot be safely discharged until that consultation is complete and its recommendations are integrated. If the nephrology consultation takes 36 hours to initiate, not because the nephrologist was unavailable, but because the communication mechanism for requesting and confirming it was broken, the patient remains admitted for an avoidable 36-hour stay.
At scale, across a physician practice or hospital system, this represents measurable and recoverable revenue loss, an occupancy inefficiency, and a patient experience failure. The American Medical Association (2024) Physician Practice Benchmark Survey identifies administrative communication overhead as one of the top contributors to physician dissatisfaction with current workflows, a finding that reflects daily experience across consultation-intensive specialties.
Preventable Readmissions
Readmission prevention depends, in part, on consultation completeness before discharge. When specialist consultation delays push clinical questions into the outpatient follow-up period, patients discharged without those questions resolved are at higher risk of readmission. Conditions requiring specialist input but were discharged without it may deteriorate during the gap between discharge and the first available outpatient appointment.
Structural communication improvements that accelerate consultation completion before discharge measurably reduce this risk. For a detailed analysis of how fragmented communication creates downstream operational costs, see our overview of the cost of fragmented clinical communication in healthcare.
The Structural Solution: Documented Real-Time Consultation
The solution to specialist consultation delay is not more specialists. It is a communication infrastructure that enables every consultation request to be initiated faster, is richer in clinical context, and is fully documented for billing and quality review.
This is precisely what CMS recognized when it established the interprofessional consultation CPT codes 99446 through 9949 and 99451 to 99452. These codes exist because telephone and internet-based consultations between treating physicians and specialists have clinical value, but that value was previously unaccounted for because the mechanism for those consultations was informal, undocumented, and unbillable. CPT 99446 covers telephonic consultations of 5 to 10 minutes. CPT 99449 covers consultations of 31 minutes or more. CPT 99451 covers the consulting specialist’s time for a written or internet-based review. CPT 99452 covers the requesting provider’s time spent initiating the written consultation. All six active codes apply to non-face-to-face, remote consultations; no patient visit is required. For a breakdown of when each code applies, see our post on telephonic vs. written interprofessional consultation.
Documentation requires a channel. The telephone does not produce documentation. ClinicianCore HCC is a secure, HIPAA-compliant, unified clinical communication platform built exclusively for physicians that creates a channel, delivering structured consultation records that satisfy both CPT billing documentation requirements and quality review standards.
ClinicianCore HCC: Faster Specialist Consultation, Documented and Billable
ClinicianCore HCC, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, replaces the phone-and-fax consultation loop with a structured workflow. Referring physicians send consultation requests with full clinical context. Specialists respond in real time or asynchronously. Both parties share a complete, auditable thread from first message to close, ready for CPT billing documentation and quality review.
How ClinicianCore HCC Reduces Specialist Consultation Turnaround Time
ClinicianCore HCC replaces the fragmented consultation initiation process with a structured workflow that reflects the realities of physician practice in 2026.
When a treating physician needs specialist input, HCC surfaces the CPT framework for that consultation at the point of initiation. The physician selects the consultation type, attaches clinical context from within the platform, and sends the request to the relevant specialist. The specialist receives the complete consultation request, patient context, clinical question, and consent acknowledgment on their device, in real time or asynchronously, depending on their availability. They respond in the same thread. Both the request and the response are documented.
For the treating physician, this eliminates phone tag. For the specialist, it eliminates compressed verbal handoffs under time pressure. For the practice, it creates a complete consultation record that supports CPT billing documentation and quality reporting. For the patient, it reduces the elapsed time between clinical need and specialist response.
The HCC ROI Calculator at cliniciancore.com allows practice administrators and medical directors to estimate the revenue recovery from documenting consultations that are currently performed informally and, if billed at all, incompletely.
Physician burnout in the clinical communication literature is partly attributed to the administrative overhead created by broken consultation workflows. Repeated phone calls, incomplete handoffs, and undocumented exchanges generate cognitive load and after-hours communication, eroding clinical capacity. A platform that structures consultation at the point of initiation not only recovers revenue, but it also recovers physician time. For an organizational view of this relationship, see our overview of the physician burnout reduction platform and the structural interventions that protect clinician capacity at scale.
Frequently Asked Questions
How long does the average specialist consultation take in US hospitals?
What is the link between specialist consultation delays and diagnostic error?
Why do specialist consultations get delayed in US hospitals?
How do communication failures cause specialist consultation delays?
How does ClinicianCore HCC reduce specialist consultation turnaround time?
References
-
- National Academies of Sciences, Engineering, and Medicine (2015). Improving Diagnosis in Health Care. Washington, DC: The National Academies Press. https://doi.org/10.17226/21794
-
- Singh H, Meyer AND, Thomas EJ (2014). The frequency of diagnostic errors in outpatient care: estimations from three large observational studies involving US adult populations. BMJ Quality and Safety, 23(9), 727-731. https://doi.org/10.1136/bmjqs-2013-002627
-
- Bates DW, Levine DM, Salmasian H, et al. (2023). The safety of inpatient health care. New England Journal of Medicine, 388(2), 142-153. https://doi.org/10.1056/NEJMsa2206117
-
- The Joint Commission (2024). Sentinel Event Data: Root Causes and Event Types. https://www.jointcommission.org/
-
- Agency for Healthcare Research and Quality (2023). Patient Safety Network: Diagnostic Safety. https://psnet.ahrq.gov/
-
- Centers for Medicare and Medicaid Services (2026). Interprofessional Consultation CPT Codes 99446-99452: Physician Fee Schedule. https://www.cms.gov/
-
- American Medical Association (2024). AMA Physician Practice Benchmark Survey. https://www.ama-assn.org/about/research/physician-practice-benchmark-survey
-
- Physicians Foundation (2023). 2023 Survey of America’s Physicians: Practice Patterns and Perspectives. https://physiciansfoundation.org/research-insights/physician-survey/