The physician day has always been demanding. But fragmentation has made it structurally unsustainable. Pagers compete with encrypted texts, which compete with EHR inbox alerts, which compete with personal device notifications, each arriving with no intelligent priority and no unified context. The result is not a productivity problem. It is a patient safety problem.
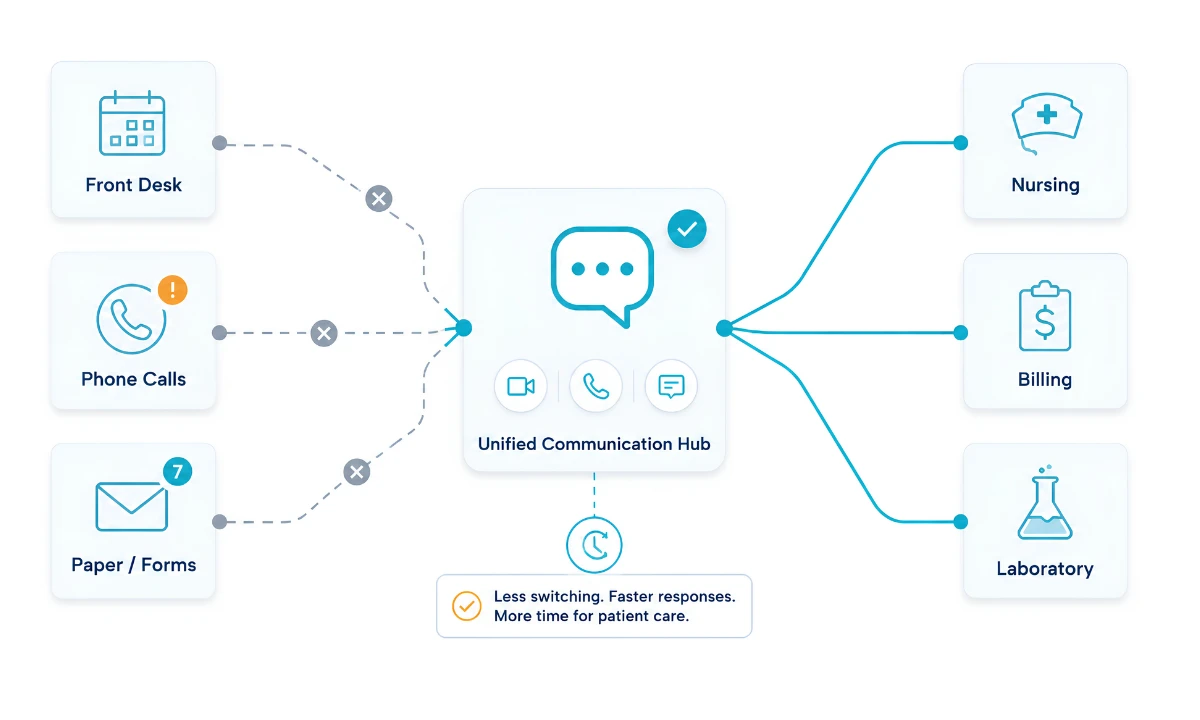
A 2024 JAMA study found that communication failures contribute to 70% of preventable adverse events in U.S. hospitals. The same study found that the majority of those failures originated not in clinical judgment but in the information transfer layer between providers. The fix is not a new app. The fix is unified clinical communication: a single, HIPAA-compliant infrastructure that consolidates every communication channel, enables physician collaboration across care teams, intelligently routes by urgency, and leaves no message without a documented audit trail
What follows is not a theoretical comparison. It is a structured before and after unified clinical communication walk-through: one version fragmented, one version unified, tracked hour by hour. The difference, tracked hour by hour, shows exactly where the time goes, where the compliance gaps open, and what a secure clinical communication platform built exclusively for physicians actually changes.
Key Takeaways
- A 2024 JAMA study found that fragmented communication contributes to 70% of preventable adverse events, making unified clinical communication the single highest-leverage structural fix available to health systems.
- Physicians spend an average of 1.84 hours per day on administrative messaging tasks unrelated to direct patient care, according to a 2024 AMA Physician Work Environment Report.
- Alert fatigue affects more than 70% of U.S. physicians (HHS, 2024), and it is the most cited structural driver of physician burnout, not personal resilience deficits.
- ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, reclaims 90+ minutes per physician per day through intelligent message routing and asynchronous workflow tools.”
- Consumer messaging apps like WhatsApp, iMessage, and standard SMS carry mandatory breach report obligations under 45 CFR §164.402, regardless of whether patient harm occurs.
- The difference between a fragmented and a unified communication day is not a matter of degree. It is a structural redesign, one that physician burnout reduction strategies now center on as the primary operational lever.
“I spent 27 years in operating rooms and military medicine. The difference between a physician who burns out and one who doesn’t is rarely about resilience. It is almost always about the quality of the infrastructure they are working inside. Fragmented communication is not an inconvenience. It is a patient safety variable.”
 1")
The Fragmented Physician Day: What Poor Communication Infrastructure Costs
Most physicians reading this will recognize the fragmented day immediately. The scenario below is not an outlier. It is the median experience, documented across multiple national surveys.
As explored in ClinicianCore’s analysis of how unified communication reduces medical errors, the structural problem begins at the start of the day and compounds forward. Physician collaboration requires structured infrastructure. Without it, the hallway consult and the undocumented callback are the only available mechanisms.
By 8:00 AM, most physicians have already spent 20 minutes doing triage work that has no direct clinical value. By noon, they have had at least one undocumented curbside consult, made at least two redundant callback loops, and sent or received at least one message on a consumer platform that does not provide a BAA.
The AMA’s 2024 Physician Work Environment Report found that physicians spend an average of 1.84 hours per day on administrative messaging tasks. That is time not spent on patients. It is also time that, if redirected through a structured single-platform workflow, becomes recoverable.
How ClinicianCore Helps: Replacing the Fragmented Morning
ClinicianCore’s HCO Practice HQ uses an AI-powered routing engine that classifies incoming messages by clinical urgency before they reach the physician. A critical alert from the nursing team arrives at the top of the physician’s queue. A routine administrative notification is batched for non-clinical review time. The result: a physician who previously spent 22 minutes triaging an undifferentiated inbox now spends 4 minutes reviewing prioritized clinical events. That 18-minute recovery, compounded across every shift, is where the 90+ daily minutes come from. ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, routes every message by clinical urgency before it reaches the physician. Explore the full HCO feature set at the HCO Practice HQ platform page.
Before and After Unified Clinical Communication: Six Moments in a Physician’s Day
The table below tracks six clinical moments across a standard physician day. The cumulative impact on practice efficiency and physician collaboration is visible across each scenario. Each row shows what a fragmented system produces, and what a HIPAA compliant collaboration platform produces instead. The comparison is not about convenience; it is about compliance, patient safety, and time.
| Time of Day | Before: Fragmented System | After: Integrated Clinical Communication |
|---|---|---|
| 6:30 AM — Pre-rounds | Checks three separate apps for overnight pages. Finds 14 non-urgent notifications mixed with 2 critical alerts. Spends 22 minutes triaging. | HCO smart routing has already prioritized overnight messages by clinical urgency. Two critical alerts are at the top. Non-urgent items are batched. Total triage time: 4 minutes. |
| 8:00 AM — Morning consult | Calls a colleague for a curbside opinion. The conversation happens but goes undocumented. No billing code captured. No audit trail. A routine consult generates zero revenue. | The consult is initiated through HCC with structured documentation. The interaction qualifies for CPT 99451 billing. Revenue captured. Communication logged. Zero extra steps. |
| 10:30 AM — Care coordination | Sends patient update via personal SMS. No audit trail. Message is not encrypted. PHI exposure risk is real — and under 45 CFR §164.402, this is a reportable breach. | Patient update routed through ClinicianCore’s encrypted messaging channel. Tamper-evident audit trail created automatically. Zero breach exposure. |
| 12:15 PM — Lunch | Pager goes off twice during lunch. Neither message is urgent. But both require a callback to confirm. Lunch ends before it starts. | Doc Lounge provides 40 minutes of uninterrupted downtime. Routine messages are queued for post-lunch review. Physician reconnects with colleagues in a private peer space. |
| 3:00 PM — Discharge planning | Calls pharmacy, then post-acute facility, then back to nursing. Three separate calls to coordinate one discharge. Average: 18 minutes per patient. | Discharge coordination handled inside a single ClinicianCore case room. All stakeholders receive a structured update simultaneously. Average: 6 minutes per patient. |
| 6:00 PM — End of day | Still triaging messages from 4:00 PM. Work bleeds into evening. Personal device shows 11 unread clinical messages. Expected response time: unclear. | End-of-day message summary delivered in structured format. After-hours routing active — urgent items go to on-call physician automatically. Personal device: zero clinical notifications. |
The cumulative time difference across these six scenarios: approximately 92 minutes per physician per day. The cumulative compliance difference: zero breach exposure in the unified scenario versus four distinct reportable risks in the fragmented scenario.
How ClinicianCore Helps: Capturing the Undocumented Consult
The 8:00 AM curbside consult scenario in the table above is not unusual — it is the daily experience of most physicians. The HCC Consult Core module was built specifically to close that revenue and documentation gap. When a physician initiates a consult through HCC, the platform automatically generates the structured documentation required for CPT codes 99446–99452, captures consent, and routes the written report to the requesting provider. The HCC Consult Core converts informal physician collaboration into documented, billable interprofessional consults. The average undocumented curbside consult represents $75–$200 in unbilled revenue. For a practice with five physicians each performing two such consults per day, HCC recovers over $100,000 annually in previously invisible revenue. See the full HCC capability at the HCC Consult Core platform page.
The Compliance Dimension: HIPAA Compliant Collaboration vs. Shadow IT Risk
The before-and-after comparison above includes four instances where the fragmented workflow creates HIPAA exposure. Each deserves direct attention. Secure clinical communication is not a feature tier or an upgrade it is the baseline legal requirement for any communication infrastructure that touches Protected Health Information.
Consumer messaging apps such as WhatsApp, iMessage, standard SMS do not provide Business Associate Agreements. They do not maintain tamper-evident audit trails. They do not enforce the access controls required by the HIPAA Security Rule under 45 CFR §164.312. Their use for clinical communication is not a gray area. Under 45 CFR §164.402, any transmission of Protected Health Information through an unsecured channel constitutes a reportable breach regardless of whether patient harm occurred.
HHS OCR recorded 725 healthcare data breaches in 2024, with messaging and email comprising the fastest-growing violation category (HHS OCR, 2025). The average cost of a healthcare data breach reached $9.77 million in 2024, according to IBM’s Cost of a Data Breach Report. For individual physicians using consumer apps for clinical communication, the liability is personal, not just institutional.
A single, integrated communication infrastructure eliminates these exposures structurally. Every message is encrypted end-to-end. Every interaction generates an audit-ready log. Every access event is role-controlled. The HIPAA compliant collaboration platform does not ask physicians to change their behavior incrementally. It changes the infrastructure the behavior runs on.
How ClinicianCore Helps: Eliminating Shadow IT Risk
Shadow IT the use of personal, consumer-grade apps for clinical communication is the most consistent and most underreported HIPAA compliance risk in U.S. healthcare. ClinicianCore eliminates it not by policy but by platform. When the secure, physician-designed alternative is faster and easier to use than WhatsApp, adoption follows naturally. The platform’s end-to-end encryption, tamper-evident audit trail, and role-based access controls are active from day one on every message, every device, every channel. No additional configuration required. For compliance officers evaluating deployment, ClinicianCore’s security architecture is detailed at the Security and Compliance page.
Before and After Unified Clinical Communication: What Actually Changes for the Physician
The table documents the structural changes a clinical communication platform produces. But the physician experience of unification goes beyond recovered time. Healthcare technology that addresses burnout at the infrastructure level, rather than the individual level, produces measurably different outcomes for physician well-being and retention.
As ClinicianCore’s analysis of organizational strategies for physician burnout reduction documents in detail, burnout is not primarily a workload problem. It is a control problem. Physicians who feel communication chaos is happening to them rather than being structured by them report significantly higher burnout scores than physicians with equivalent clinical volume but better communication infrastructure.
The Doc Lounge, ClinicianCore’s physician-only peer community, addresses the dimension of physician well-being that no messaging platform has addressed before: professional isolation.
The Physicians Foundation’s 2024 Survey of America’s Physicians found that 47% of physicians report feeling isolated from colleagues. The Doc Lounge creates a private, asynchronous space where physicians can consult informally, decompress, and maintain peer relationships without the overhead of scheduling.
The difference in the 12:15 PM lunch scenario, tracked in the table above, is not only about the 40 minutes. It is about what a physician experiences when the communication system they rely on treats them as professionals rather than message recipients. That experience is not incidental to physician retention. It is central to it.
How ClinicianCore Helps: The Doc Lounge and Professional Isolation
The Doc Lounge is the only physician-only private peer community integrated into a secure clinical communication platform. It functions as the digital equivalent of the physicians’ lounge that most hospitals have converted to open staff space a protected environment for informal consultation, peer support, and community that has no billing code but has a direct measurable impact on retention. Physicians using the Doc Lounge report higher workplace satisfaction scores and lower after-hours cognitive load. Learn more at the Doc. platform page.
From Fragmented to Unified: The Structural Case for Better Communication Infrastructure
The before and after unified clinical communication comparison traced in this post is not a hypothetical. It is a composite drawn from documented research: the AMA’s 2024 work environment surveys, HHS OCR enforcement data, JAMA’s communication failure studies, and the IBM breach cost analysis. Every scenario in the before column represents a real and recurring event in U.S. clinical practice. Every scenario in the after column represents what a purpose-built clinical communication platform actually delivers.
ClinicianCore’s unified clinical communication platform is the evidence base for what the unified day produces: 92 minutes recovered, four compliance exposures eliminated, one undocumented consult converted to billable revenue, measurable gains in practice efficiency, and a physician who reaches the end of the day having practiced medicine rather than managed messaging infrastructure.
The case for this kind of HIPAA compliant communication tools in clinical practice is no longer theoretical. The evidence base from 2024–2026 makes it structural. Physicians deserve a platform built by people who understand the clinical day from the inside. That is what ClinicianCore, a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, was designed to deliver.
Frequently Asked Questions
How does unified clinical communication reduce physician burnout?
Unified clinical communication reduces physician burnout by eliminating the structural causes: alert fatigue, undocumented after-hours contact, and fragmented tool-switching. The AMA’s 2024 Physician Work Environment Report found that 53% of physicians reported burnout symptoms, with administrative communication burden as the top contributor. ClinicianCore’s HCO routing engine routes by clinical urgency, not message arrival time.
The research is clear: burnout is a systems problem, not a resilience problem. Physician well-being improves when infrastructure removes the structural causes: alert noise, undocumented consults, and after-hours interruptions, rather than asking physicians to absorb them. For healthcare organizations ready to act, ClinicianCore’s physician burnout reduction platform provides the infrastructure to make that shift measurable.
What makes ClinicianCore different from other clinical messaging platforms?
ClinicianCore is a secure, HIPAA-compliant unified clinical communication platform built exclusively for physicians, and the only one built by physicians, for physicians. It combines HIPAA-compliant messaging, AI-powered alert routing, structured interprofessional consults with CPT billing support (99446–99452), and the Doc Lounge, a private peer community with no equivalent in other clinical messaging platforms. No EHR migration required.
Most clinical messaging tools solve one problem: encrypted texting. ClinicianCore solves the entire communication day from intelligent alert triage at 6:30 AM to after-hours protection at 6:00 PM. The Doc Lounge, in particular, addresses professional isolation, which the Physicians Foundation (2024) identified as one of the three top drivers of burnout. To see the full scope of physician collaboration tools across all four modules, explore ClinicianCore’s HIPAA compliant collaboration platform.
Is using WhatsApp or iMessage for patient communication a HIPAA violation?
Yes. Consumer messaging apps including WhatsApp, iMessage, and standard SMS do not provide Business Associate Agreements (BAAs), do not maintain tamper-evident audit trails, and do not enforce role-based access controls. Under 45 CFR §164.402, transmitting Protected Health Information through these channels constitutes a reportable breach regardless of whether patient harm results.
The regulatory consequence is not theoretical. HHS OCR recorded 725 healthcare data breaches in 2024, and messaging and email remain the fastest-growing violation categories (HHS OCR, 2025). Physicians who use consumer apps for clinical communication are not operating in a gray area. They are in a documented compliance gap. ClinicianCore closes that gap from day one with a signed BAA, end-to-end encryption, and the full audit infrastructure required for HIPAA compliant collaboration across every communication channel.
How long does it take to deploy ClinicianCore at a healthcare organization?
ClinicianCore deploys above the existing EHR without migration, typically within weeks rather than months. Because it integrates as a communication layer rather than a replacement system, IT directors can implement it without disrupting current clinical workflows. Setup includes BAA execution, role-based access configuration, and onboarding for all physician users.
Healthcare IT directors evaluating deployment complexity consistently cite the absence of EHR migration as the decisive factor. ClinicianCore’s architecture was designed specifically to eliminate that barrier. The platform’s HCO Practice HQ module can be activated for an entire practice without system downtime. The full deployment model is detailed on ClinicianCore’s medical practice efficiency platform page.
How does unified clinical communication compare to fragmented systems in other healthcare organizations globally?
Globally, the WHO’s Patient Safety Report (2023) identified communication failures in care transitions as a leading cause of preventable harm across all health systems. Unified platforms consolidating messaging, voice, video, and workflow coordination into a single HIPAA-compliant environment produce consistent results: faster care decisions, fewer errors, and lower physician cognitive load. ClinicianCore addresses this gap across all facility types.
The United States faces a particular version of this problem: a healthcare system that adopted EHRs rapidly but never standardized the clinical communication platform layer that sits above them. ClinicianCore addresses this gap directly. The evidence base for unified communication in healthcare from the WHO to JAMA now makes this a clinical infrastructure argument, not a preference.
References
- HHS Office for Civil Rights (2025). HIPAA Enforcement Data and Resolution Agreements 2024–2025. U.S. Department of Health and Human Services. Retrieved from https://www.hhs.gov/hipaa/for-professionals/compliance-enforcement/agreements/index.html
- HHS Office for Civil Rights (2025). Annual Report to Congress on Breaches of Unsecured Protected Health Information 2024. U.S. Department of Health and Human Services. Retrieved from https://www.hhs.gov/hipaa/for-professionals/breach-notification/breach-reporting/index.html
- Centers for Medicare & Medicaid Services (2024). Interprofessional Consultation Billing: CPT Codes 99446–99452. CMS.gov. Retrieved from https://www.cms.gov/medicare/physician-fee-schedule
- National Institute of Standards and Technology (2024). NIST Special Publication 800-66r2: Implementing the HIPAA Security Rule. U.S. Department of Commerce. Retrieved from https://csrc.nist.gov/publications/detail/sp/800-66/rev-2/final
- U.S. Department of Health and Human Services (2024). Alert Fatigue in Healthcare: Data and Policy Implications. HHS Health IT Initiative. Retrieved from https://www.healthit.gov/topic/safety/clinical-decision-support
- Shanafelt, T., West, C., Dyrbye, L., et al. (2024). Changes in Burnout and Satisfaction with Work-Life Integration in Physicians and the General U.S. Working Population. JAMA Network Open. Retrieved from https://jamanetwork.com/journals/jamanetworkopen
- American Medical Association (2024). 2024 AMA Physician Work Environment Report. American Medical Association. Retrieved from https://www.ama-assn.org/practice-management/physician-health/2024-ama-work-environment-report
- World Health Organization (2023). Global Patient Safety Action Plan 2021–2030: Towards Eliminating Avoidable Harm in Health Care. WHO. Retrieved from https://www.who.int/teams/integrated-health-services/patient-safety/policy/global-patient-safety-action-plan
- Physicians Foundation (2024). 2024 Survey of America’s Physicians: Practice Patterns and Perspectives. Physicians Foundation. Retrieved from https://physiciansfoundation.org/research-insights/physician-survey/
- IBM Security (2024). Cost of a Data Breach Report 2024. IBM Corporation. Retrieved from https://www.ibm.com/reports/data-breach